{"title":"高危壶腹周围憩室的临床及ct特征。","authors":"Jun-Wei Gong, Tian-You Luo, Jiao Zhang, Zhu Zhang, Xin-Mei Wang, Qi Li","doi":"10.21037/qims-2024-2501","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Periampullary diverticulum (PAD) is a common acquired extraluminal outpouching of duodenal mucosa and is often clinically overlooked. When complicated by biliary-pancreatic stones or inflammation, PAD may lead to severe biliary-pancreatic complications. Although endoscopic retrograde cholangiopancreatography (ERCP) is currently regarded as the gold standard for PAD diagnosis, its invasive nature and other limitations have led to computed tomography (CT) being increasingly preferred as the first-line imaging modality. However, the correlation between imaging features and clinical manifestations remains unclear for high-risk PAD (HRPAD), defined as PAD associated with cholelithiasis and biliary-pancreatic inflammation. Therefore, this study aimed to examine the clinical and CT characteristics of HRPAD.</p><p><strong>Methods: </strong>The data of 260 patients with HRPAD and 288 patients with non-high-risk PAD (N-HRPAD) who underwent contrast-enhanced abdominal CT scans between January 2018 and May 2024 were retrospectively analyzed. The clinical and CT features were compared between the groups. Independent factors for diagnosing HRPAD were identified through binary logistic regression analysis. Additionally, an external validation cohort comprising 150 patients from another center was used to test the predictive efficiency of the model.</p><p><strong>Results: </strong>Patients with HRPAD were significantly older than those with N-HRPAD, with an average age of 72±10 and 68±11 years, respectively (P<0.001). Additionally, they exhibited a higher proportion of larger diverticula (>1.95 cm: 65.38% <i>vs</i>. 22.57%), larger common bile duct (CBD) size (>0.69 cm: 72.31% <i>vs</i>. 20.83%), and greater pancreatic duct (PD) dilation (>0.20 cm: 86.92% <i>vs</i>. 60.42%) (all P values <0.001). Furthermore, there was a greater prevalence of diverticular neck swelling in the HRPAD group than in the control group (23.08% <i>vs</i>. 4.86%; P<0.001). Binary logistic regression analysis indicated that a diverticulum size >1.95 cm, CBD size >0.69 cm, PD size >0.20 cm, and the presence of diverticular neck swelling were predictors significantly associated with HRPAD, yielding an area under the curve (AUC) of 0.848; meanwhile, the AUC of the external validation cohort was 0.829.</p><p><strong>Conclusions: </strong>Patients with HRPAD and those with N-HRPAD exhibited different clinical and imaging characteristics. A thorough understanding of these differences may facilitate early identification of HRPAD and timely treatment interventions, which would reduce complications related to biliary-pancreatic diseases.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8239-8249"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397622/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical and computed tomography characteristics of high-risk periampullary diverticulum.\",\"authors\":\"Jun-Wei Gong, Tian-You Luo, Jiao Zhang, Zhu Zhang, Xin-Mei Wang, Qi Li\",\"doi\":\"10.21037/qims-2024-2501\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Periampullary diverticulum (PAD) is a common acquired extraluminal outpouching of duodenal mucosa and is often clinically overlooked. When complicated by biliary-pancreatic stones or inflammation, PAD may lead to severe biliary-pancreatic complications. Although endoscopic retrograde cholangiopancreatography (ERCP) is currently regarded as the gold standard for PAD diagnosis, its invasive nature and other limitations have led to computed tomography (CT) being increasingly preferred as the first-line imaging modality. However, the correlation between imaging features and clinical manifestations remains unclear for high-risk PAD (HRPAD), defined as PAD associated with cholelithiasis and biliary-pancreatic inflammation. Therefore, this study aimed to examine the clinical and CT characteristics of HRPAD.</p><p><strong>Methods: </strong>The data of 260 patients with HRPAD and 288 patients with non-high-risk PAD (N-HRPAD) who underwent contrast-enhanced abdominal CT scans between January 2018 and May 2024 were retrospectively analyzed. The clinical and CT features were compared between the groups. Independent factors for diagnosing HRPAD were identified through binary logistic regression analysis. Additionally, an external validation cohort comprising 150 patients from another center was used to test the predictive efficiency of the model.</p><p><strong>Results: </strong>Patients with HRPAD were significantly older than those with N-HRPAD, with an average age of 72±10 and 68±11 years, respectively (P<0.001). Additionally, they exhibited a higher proportion of larger diverticula (>1.95 cm: 65.38% <i>vs</i>. 22.57%), larger common bile duct (CBD) size (>0.69 cm: 72.31% <i>vs</i>. 20.83%), and greater pancreatic duct (PD) dilation (>0.20 cm: 86.92% <i>vs</i>. 60.42%) (all P values <0.001). Furthermore, there was a greater prevalence of diverticular neck swelling in the HRPAD group than in the control group (23.08% <i>vs</i>. 4.86%; P<0.001). Binary logistic regression analysis indicated that a diverticulum size >1.95 cm, CBD size >0.69 cm, PD size >0.20 cm, and the presence of diverticular neck swelling were predictors significantly associated with HRPAD, yielding an area under the curve (AUC) of 0.848; meanwhile, the AUC of the external validation cohort was 0.829.</p><p><strong>Conclusions: </strong>Patients with HRPAD and those with N-HRPAD exhibited different clinical and imaging characteristics. A thorough understanding of these differences may facilitate early identification of HRPAD and timely treatment interventions, which would reduce complications related to biliary-pancreatic diseases.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 9\",\"pages\":\"8239-8249\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397622/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-2024-2501\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2024-2501","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:壶腹周围憩室(PAD)是一种常见的获得性十二指肠粘膜腔外突出,临床上常被忽视。当并发胆胰结石或炎症时,PAD可导致严重的胆胰并发症。虽然内窥镜逆行胰胆管造影(ERCP)目前被认为是PAD诊断的金标准,但其侵入性和其他局限性使得计算机断层扫描(CT)越来越多地被首选为一线成像方式。然而,高危PAD (HRPAD)的影像学特征与临床表现之间的相关性尚不清楚,定义为伴有胆石症和胆胰炎症的PAD。因此,本研究旨在探讨HRPAD的临床和CT特征。方法:回顾性分析2018年1月至2024年5月260例HRPAD患者和288例非高危PAD (N-HRPAD)患者行腹部CT增强扫描的资料。比较两组患者的临床及CT表现。通过二元logistic回归分析确定诊断HRPAD的独立因素。此外,一个由来自另一个中心的150名患者组成的外部验证队列被用来测试该模型的预测效率。结果:HRPAD患者明显大于N-HRPAD患者,平均年龄分别为72±10岁和68±11岁(P1.95 cm: 65.38% vs. 22.57%),总胆管(CBD)尺寸较大(>0.69 cm: 72.31% vs. 20.83%),胰管(PD)扩张较大(>0.20 cm: 86.92% vs. 60.42%) (P值均为4.86%;P1.95 cm、CBD大小>0.69 cm、PD大小>0.20 cm、是否存在憩室性颈部肿胀是与HRPAD显著相关的预测因子,曲线下面积(AUC)为0.848;外部验证队列的AUC为0.829。结论:HRPAD患者与N-HRPAD患者表现出不同的临床和影像学特征。深入了解这些差异可能有助于HRPAD的早期识别和及时的治疗干预,从而减少胆胰疾病相关的并发症。
Clinical and computed tomography characteristics of high-risk periampullary diverticulum.
Background: Periampullary diverticulum (PAD) is a common acquired extraluminal outpouching of duodenal mucosa and is often clinically overlooked. When complicated by biliary-pancreatic stones or inflammation, PAD may lead to severe biliary-pancreatic complications. Although endoscopic retrograde cholangiopancreatography (ERCP) is currently regarded as the gold standard for PAD diagnosis, its invasive nature and other limitations have led to computed tomography (CT) being increasingly preferred as the first-line imaging modality. However, the correlation between imaging features and clinical manifestations remains unclear for high-risk PAD (HRPAD), defined as PAD associated with cholelithiasis and biliary-pancreatic inflammation. Therefore, this study aimed to examine the clinical and CT characteristics of HRPAD.
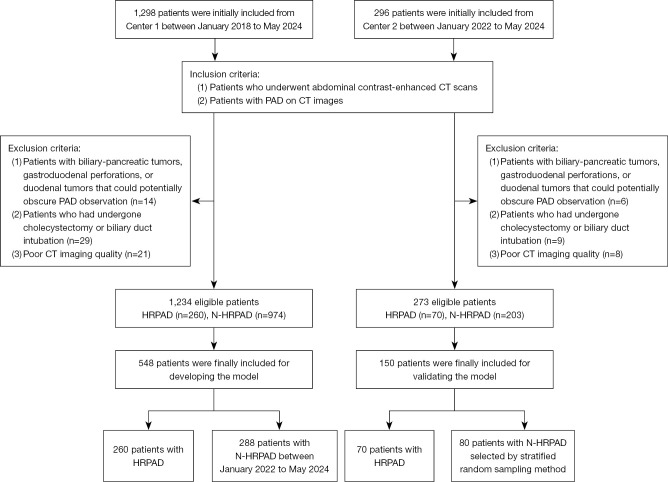
Methods: The data of 260 patients with HRPAD and 288 patients with non-high-risk PAD (N-HRPAD) who underwent contrast-enhanced abdominal CT scans between January 2018 and May 2024 were retrospectively analyzed. The clinical and CT features were compared between the groups. Independent factors for diagnosing HRPAD were identified through binary logistic regression analysis. Additionally, an external validation cohort comprising 150 patients from another center was used to test the predictive efficiency of the model.
Results: Patients with HRPAD were significantly older than those with N-HRPAD, with an average age of 72±10 and 68±11 years, respectively (P<0.001). Additionally, they exhibited a higher proportion of larger diverticula (>1.95 cm: 65.38% vs. 22.57%), larger common bile duct (CBD) size (>0.69 cm: 72.31% vs. 20.83%), and greater pancreatic duct (PD) dilation (>0.20 cm: 86.92% vs. 60.42%) (all P values <0.001). Furthermore, there was a greater prevalence of diverticular neck swelling in the HRPAD group than in the control group (23.08% vs. 4.86%; P<0.001). Binary logistic regression analysis indicated that a diverticulum size >1.95 cm, CBD size >0.69 cm, PD size >0.20 cm, and the presence of diverticular neck swelling were predictors significantly associated with HRPAD, yielding an area under the curve (AUC) of 0.848; meanwhile, the AUC of the external validation cohort was 0.829.
Conclusions: Patients with HRPAD and those with N-HRPAD exhibited different clinical and imaging characteristics. A thorough understanding of these differences may facilitate early identification of HRPAD and timely treatment interventions, which would reduce complications related to biliary-pancreatic diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


