Aleksi K Winstén, Ville Langén, K E Juhani Airaksinen, Konsta Teppo
{"title":"估计心房颤动患者口服非维生素K拮抗剂抗凝的卒中风险阈值:马尔可夫决策模型分析。","authors":"Aleksi K Winstén, Ville Langén, K E Juhani Airaksinen, Konsta Teppo","doi":"10.1161/CIRCOUTCOMES.125.012090","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Randomized trials have clearly demonstrated the benefits of anticoagulant therapy in patients with atrial fibrillation who are at high risk of ischemic stroke. However, less is known about the benefit of anticoagulation in low-risk patients, and exactly how low baseline stroke risk justifies further attempts to reduce it with direct oral anticoagulants (DOACs) remains unclear.</p><p><strong>Methods: </strong>We developed a Markov decision model to estimate the impact of initiating DOACs on quality-adjusted life years (QALYs) on a 20-year time horizon in patients with atrial fibrillation across a range of nonanticoagulated ischemic stroke risk. The model incorporated data from randomized controlled trials on the effects of DOACs on the severity and risk of ischemic stroke, major bleeding, and mortality, as well as previous evidence on their impact on quality of life. Nonanticoagulated event rates were averaged from previous observational studies.</p><p><strong>Results: </strong>The tipping point in the annual nonanticoagulated ischemic stroke rate, at which DOAC treatment resulted in equal cumulative QALYs as withholding therapy, was 0.65%. Below this risk threshold, DOAC therapy yielded slightly fewer QALYs, while, above it, DOAC therapy resulted in increasingly higher QALYs. At nonanticoagulated stroke risk levels of 1%, 2%, and 3%, the mean QALY gains with DOACs per patient during a 20-year simulation were 0.13, 0.53, and 1.00, respectively, whereas, at the stroke risk level of 0.4%, DOAC therapy resulted in 0.01 lower QALYs per patient.</p><p><strong>Conclusions: </strong>In this simulation, DOAC therapy versus no anticoagulation was associated with a net benefit on QALYs in patients with atrial fibrillation with an annual nonanticoagulated stroke risk >0.65%, with the magnitude of benefit increasing with higher stroke risk.</p>","PeriodicalId":49221,"journal":{"name":"Circulation-Cardiovascular Quality and Outcomes","volume":" ","pages":"e012090"},"PeriodicalIF":6.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442775/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimating the Stroke Risk Threshold for Initiating Non-Vitamin K Antagonist Oral Anticoagulation in Atrial Fibrillation: Markov Decision Model Analysis.\",\"authors\":\"Aleksi K Winstén, Ville Langén, K E Juhani Airaksinen, Konsta Teppo\",\"doi\":\"10.1161/CIRCOUTCOMES.125.012090\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Randomized trials have clearly demonstrated the benefits of anticoagulant therapy in patients with atrial fibrillation who are at high risk of ischemic stroke. However, less is known about the benefit of anticoagulation in low-risk patients, and exactly how low baseline stroke risk justifies further attempts to reduce it with direct oral anticoagulants (DOACs) remains unclear.</p><p><strong>Methods: </strong>We developed a Markov decision model to estimate the impact of initiating DOACs on quality-adjusted life years (QALYs) on a 20-year time horizon in patients with atrial fibrillation across a range of nonanticoagulated ischemic stroke risk. The model incorporated data from randomized controlled trials on the effects of DOACs on the severity and risk of ischemic stroke, major bleeding, and mortality, as well as previous evidence on their impact on quality of life. Nonanticoagulated event rates were averaged from previous observational studies.</p><p><strong>Results: </strong>The tipping point in the annual nonanticoagulated ischemic stroke rate, at which DOAC treatment resulted in equal cumulative QALYs as withholding therapy, was 0.65%. Below this risk threshold, DOAC therapy yielded slightly fewer QALYs, while, above it, DOAC therapy resulted in increasingly higher QALYs. At nonanticoagulated stroke risk levels of 1%, 2%, and 3%, the mean QALY gains with DOACs per patient during a 20-year simulation were 0.13, 0.53, and 1.00, respectively, whereas, at the stroke risk level of 0.4%, DOAC therapy resulted in 0.01 lower QALYs per patient.</p><p><strong>Conclusions: </strong>In this simulation, DOAC therapy versus no anticoagulation was associated with a net benefit on QALYs in patients with atrial fibrillation with an annual nonanticoagulated stroke risk >0.65%, with the magnitude of benefit increasing with higher stroke risk.</p>\",\"PeriodicalId\":49221,\"journal\":{\"name\":\"Circulation-Cardiovascular Quality and Outcomes\",\"volume\":\" \",\"pages\":\"e012090\"},\"PeriodicalIF\":6.7000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442775/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation-Cardiovascular Quality and Outcomes\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1161/CIRCOUTCOMES.125.012090\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation-Cardiovascular Quality and Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/CIRCOUTCOMES.125.012090","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Estimating the Stroke Risk Threshold for Initiating Non-Vitamin K Antagonist Oral Anticoagulation in Atrial Fibrillation: Markov Decision Model Analysis.
Background: Randomized trials have clearly demonstrated the benefits of anticoagulant therapy in patients with atrial fibrillation who are at high risk of ischemic stroke. However, less is known about the benefit of anticoagulation in low-risk patients, and exactly how low baseline stroke risk justifies further attempts to reduce it with direct oral anticoagulants (DOACs) remains unclear.
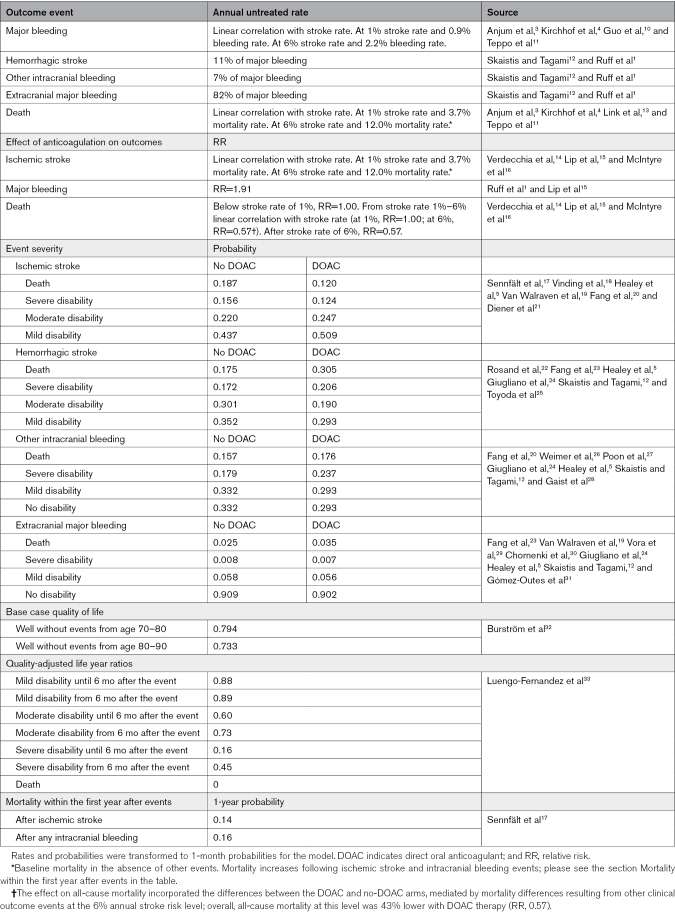
Methods: We developed a Markov decision model to estimate the impact of initiating DOACs on quality-adjusted life years (QALYs) on a 20-year time horizon in patients with atrial fibrillation across a range of nonanticoagulated ischemic stroke risk. The model incorporated data from randomized controlled trials on the effects of DOACs on the severity and risk of ischemic stroke, major bleeding, and mortality, as well as previous evidence on their impact on quality of life. Nonanticoagulated event rates were averaged from previous observational studies.
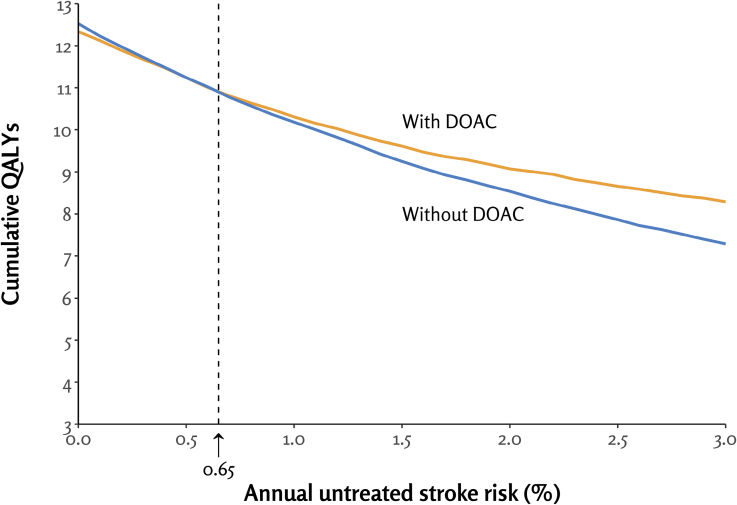
Results: The tipping point in the annual nonanticoagulated ischemic stroke rate, at which DOAC treatment resulted in equal cumulative QALYs as withholding therapy, was 0.65%. Below this risk threshold, DOAC therapy yielded slightly fewer QALYs, while, above it, DOAC therapy resulted in increasingly higher QALYs. At nonanticoagulated stroke risk levels of 1%, 2%, and 3%, the mean QALY gains with DOACs per patient during a 20-year simulation were 0.13, 0.53, and 1.00, respectively, whereas, at the stroke risk level of 0.4%, DOAC therapy resulted in 0.01 lower QALYs per patient.
Conclusions: In this simulation, DOAC therapy versus no anticoagulation was associated with a net benefit on QALYs in patients with atrial fibrillation with an annual nonanticoagulated stroke risk >0.65%, with the magnitude of benefit increasing with higher stroke risk.
期刊介绍:
Circulation: Cardiovascular Quality and Outcomes, an American Heart Association journal, publishes articles related to improving cardiovascular health and health care. Content includes original research, reviews, and case studies relevant to clinical decision-making and healthcare policy. The online-only journal is dedicated to furthering the mission of promoting safe, effective, efficient, equitable, timely, and patient-centered care. Through its articles and contributions, the journal equips you with the knowledge you need to improve clinical care and population health, and allows you to engage in scholarly activities of consequence to the health of the public. Circulation: Cardiovascular Quality and Outcomes considers the following types of articles: Original Research Articles, Data Reports, Methods Papers, Cardiovascular Perspectives, Care Innovations, Novel Statistical Methods, Policy Briefs, Data Visualizations, and Caregiver or Patient Viewpoints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


