Julia Chapon, Julien Scanzi, Harry Sokol, Bruno Pereira, Anthony Buisson
{"title":"不同方式粪便菌群移植治疗溃疡性结肠炎的疗效:系统评价和网络荟萃分析。","authors":"Julia Chapon, Julien Scanzi, Harry Sokol, Bruno Pereira, Anthony Buisson","doi":"10.1177/17562848251369624","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While several small sample size randomized controlled trials suggested the superiority of faecal microbiota transplantation (FMT) over placebo in ulcerative colitis (UC), the most effective modality to perform FMT remains unknown.</p><p><strong>Objectives: </strong>To compare the efficacy of different modalities of FMT to induce clinical remission in patients with UC.</p><p><strong>Data sources and methods: </strong>We performed a systematic review and network analysis (sources: MEDLINE, Embase, Cochrane CENTRAL; random effects model) of randomized controlled trials including at least one arm of FMT in adult patients with active UC. The primary endpoint, that is, clinical remission (total Mayo score ⩽2 with Mayo endoscopic score ⩽1), was assessed between weeks 6 and 12. Results are expressed as relative risks with 95% confidence intervals, adjusted for bowel cleansing and pre-FMT antibiotics. Ranking of FMT modalities was calculated as their surface under the cumulative ranking (SUCRA).</p><p><strong>Results: </strong>Among the 12 selected studies, patients were exclusively bio-naïve in 4 studies (4/12), while between 9% and 32% had prior biologics exposure in the other trials. The risk of bias was low across all domains in seven studies. Contrary to upper gastrointestinal tract (GI) FMT (Relative risk (RR) = 1.1 (0.2-7.7)), oral capsule (RR = 7.1 (1.8-33.3)), lower GI FMT (RR = 4.5 (1.7-12.5) and combination of both (RR = 12.5 (2.1-100)) are more effective than placebo to induce clinical remission. The combination of lower GI FMT and oral capsule was significantly more effective than upper GI FMT to induce clinical remission (RR = 10.7 (1.1-104.2)). Combination of lower GI FMT and oral capsule ranked the highest for the induction of clinical remission (SUCRA = 0.93). Multidonor FMT did not perform better than single donor FMT. Autologous FMT ranked lower than placebo (SUCRA = 0.12 vs 0.22).</p><p><strong>Conclusion: </strong>The combination of lower GI and oral capsule FMT seems to be the best modality of FMT for patients with UC. In clinical trials, autologous FMT should be avoided due to a potential detrimental effect.</p><p><strong>Trial registration: </strong>PROSPERO registration number: CRD42023385511.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251369624"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378343/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy of different modalities of faecal microbiota transplantation in ulcerative colitis: systematic review and network meta-analysis.\",\"authors\":\"Julia Chapon, Julien Scanzi, Harry Sokol, Bruno Pereira, Anthony Buisson\",\"doi\":\"10.1177/17562848251369624\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While several small sample size randomized controlled trials suggested the superiority of faecal microbiota transplantation (FMT) over placebo in ulcerative colitis (UC), the most effective modality to perform FMT remains unknown.</p><p><strong>Objectives: </strong>To compare the efficacy of different modalities of FMT to induce clinical remission in patients with UC.</p><p><strong>Data sources and methods: </strong>We performed a systematic review and network analysis (sources: MEDLINE, Embase, Cochrane CENTRAL; random effects model) of randomized controlled trials including at least one arm of FMT in adult patients with active UC. The primary endpoint, that is, clinical remission (total Mayo score ⩽2 with Mayo endoscopic score ⩽1), was assessed between weeks 6 and 12. Results are expressed as relative risks with 95% confidence intervals, adjusted for bowel cleansing and pre-FMT antibiotics. Ranking of FMT modalities was calculated as their surface under the cumulative ranking (SUCRA).</p><p><strong>Results: </strong>Among the 12 selected studies, patients were exclusively bio-naïve in 4 studies (4/12), while between 9% and 32% had prior biologics exposure in the other trials. The risk of bias was low across all domains in seven studies. Contrary to upper gastrointestinal tract (GI) FMT (Relative risk (RR) = 1.1 (0.2-7.7)), oral capsule (RR = 7.1 (1.8-33.3)), lower GI FMT (RR = 4.5 (1.7-12.5) and combination of both (RR = 12.5 (2.1-100)) are more effective than placebo to induce clinical remission. The combination of lower GI FMT and oral capsule was significantly more effective than upper GI FMT to induce clinical remission (RR = 10.7 (1.1-104.2)). Combination of lower GI FMT and oral capsule ranked the highest for the induction of clinical remission (SUCRA = 0.93). Multidonor FMT did not perform better than single donor FMT. Autologous FMT ranked lower than placebo (SUCRA = 0.12 vs 0.22).</p><p><strong>Conclusion: </strong>The combination of lower GI and oral capsule FMT seems to be the best modality of FMT for patients with UC. In clinical trials, autologous FMT should be avoided due to a potential detrimental effect.</p><p><strong>Trial registration: </strong>PROSPERO registration number: CRD42023385511.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"18 \",\"pages\":\"17562848251369624\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-08-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378343/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848251369624\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251369624","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Efficacy of different modalities of faecal microbiota transplantation in ulcerative colitis: systematic review and network meta-analysis.
Background: While several small sample size randomized controlled trials suggested the superiority of faecal microbiota transplantation (FMT) over placebo in ulcerative colitis (UC), the most effective modality to perform FMT remains unknown.
Objectives: To compare the efficacy of different modalities of FMT to induce clinical remission in patients with UC.
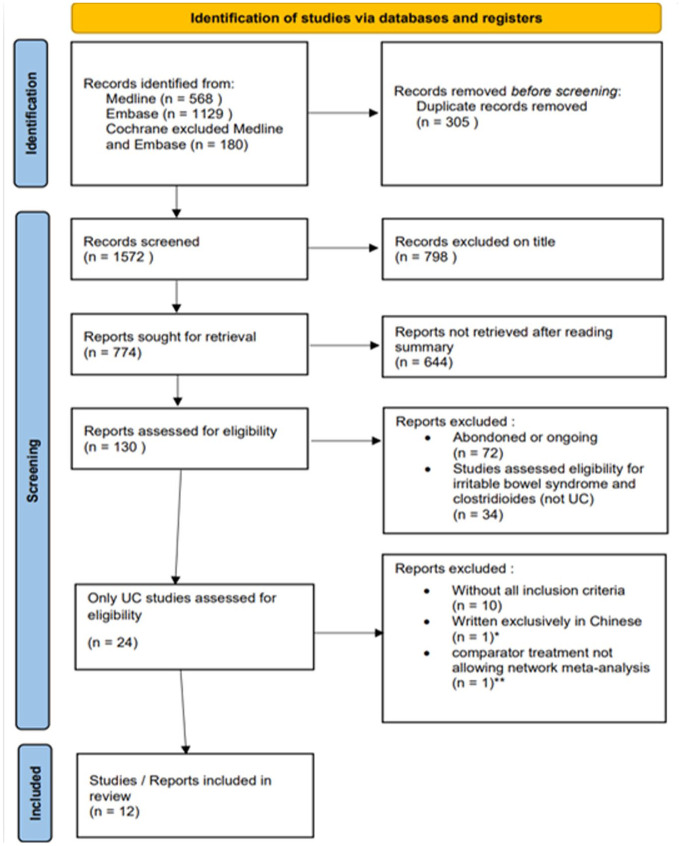
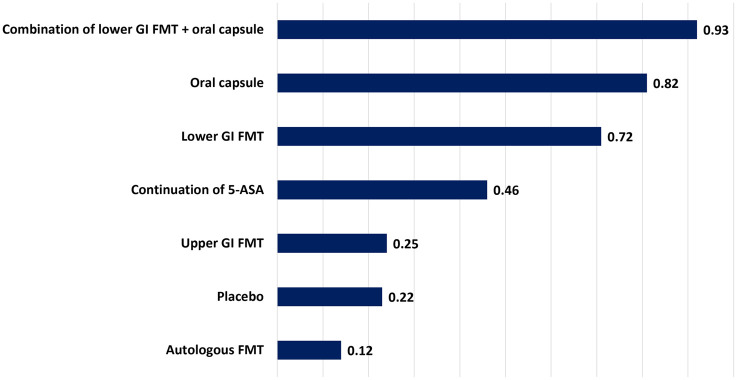
Data sources and methods: We performed a systematic review and network analysis (sources: MEDLINE, Embase, Cochrane CENTRAL; random effects model) of randomized controlled trials including at least one arm of FMT in adult patients with active UC. The primary endpoint, that is, clinical remission (total Mayo score ⩽2 with Mayo endoscopic score ⩽1), was assessed between weeks 6 and 12. Results are expressed as relative risks with 95% confidence intervals, adjusted for bowel cleansing and pre-FMT antibiotics. Ranking of FMT modalities was calculated as their surface under the cumulative ranking (SUCRA).
Results: Among the 12 selected studies, patients were exclusively bio-naïve in 4 studies (4/12), while between 9% and 32% had prior biologics exposure in the other trials. The risk of bias was low across all domains in seven studies. Contrary to upper gastrointestinal tract (GI) FMT (Relative risk (RR) = 1.1 (0.2-7.7)), oral capsule (RR = 7.1 (1.8-33.3)), lower GI FMT (RR = 4.5 (1.7-12.5) and combination of both (RR = 12.5 (2.1-100)) are more effective than placebo to induce clinical remission. The combination of lower GI FMT and oral capsule was significantly more effective than upper GI FMT to induce clinical remission (RR = 10.7 (1.1-104.2)). Combination of lower GI FMT and oral capsule ranked the highest for the induction of clinical remission (SUCRA = 0.93). Multidonor FMT did not perform better than single donor FMT. Autologous FMT ranked lower than placebo (SUCRA = 0.12 vs 0.22).
Conclusion: The combination of lower GI and oral capsule FMT seems to be the best modality of FMT for patients with UC. In clinical trials, autologous FMT should be avoided due to a potential detrimental effect.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


