Jiajia Xu, Chao Chen, Yanhua Ye, Yanqiao Ren, Ke Chen, Guofeng Zhou, Chuan Cheng, Yuexiang Peng
{"title":"不可切除胆管癌合并梗阻性黄疸合并经皮经肝胆管引流联合DEB-TACE治疗的疗效:与单纯DEB-TACE比较。","authors":"Jiajia Xu, Chao Chen, Yanhua Ye, Yanqiao Ren, Ke Chen, Guofeng Zhou, Chuan Cheng, Yuexiang Peng","doi":"10.1177/17562848251360114","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intrahepatic cholangiocarcinoma (ICC) with obstructive jaundice presents a therapeutic challenge, as most patients are ineligible for surgery. While FOLFOX chemotherapy offers limited survival benefits, drug-eluting bead transarterial chemoembolization (DEB-TACE) combined with percutaneous transhepatic cholangial drainage (PTCD) may improve outcomes by addressing both tumor burden and biliary obstruction.</p><p><strong>Objective: </strong>To evaluate the efficacy and safety of DEB-TACE + PTCD versus DEB-TACE alone in unresectable ICC patients with obstructive jaundice.</p><p><strong>Design: </strong>Retrospective cohort study of 209 patients treated between January 2015 and November 2024.</p><p><strong>Methods: </strong>A total of 209 patients with ICC and obstructive jaundice were included, with 95 patients in the DEB-TACE + PTCD group (D + P group) and 114 patients in the DEB-TACE alone group (DEB group). Tumor responses were evaluated at 3 months to assess treatment efficacy, while statistical analyses of adverse events were conducted to evaluate treatment safety. Kaplan-Meier method was utilized to generate survival curves. Cox analysis was performed to identify factors influencing prognosis.</p><p><strong>Results: </strong>The median progression-free survival and OS were 6 and 14 months in D + P group and 5 and 11 months in the DEB group. The 3-month objective response rate (ORR) and disease control rate (DCR) were 36.2% and 76.6% in the D + P group. While in the DEB group, the ORR and DCR were 34.2% (<i>p</i> = 0.772) and 62.2% (<i>p</i> = 0.026). Multivariate Cox regression analysis revealed that lymph node metastasis (hazard ratio (HR) = 0.727, confidence interval (CI: 0.535-0.987), <i>p</i> = 0.041), level of cancer antigen (CA)-125 (HR = 0.670, CI (0.503-0.894), <i>p</i> = 0.006), and treatment (HR = 1.335, CI (1.002-1.780), <i>p</i> = 0.049) were predictors for prognosis.</p><p><strong>Conclusion: </strong>For patients with unresectable cholangiocarcinoma complicated by obstructive jaundice, DEB-TACE following PTCD may be a safer and more effective treatment.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251360114"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374100/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcome of adding percutaneous transhepatic cholangial drainage to DEB-TACE in patients with unresectable cholangiocarcinoma with obstructive jaundice: comparison with sole DEB-TACE.\",\"authors\":\"Jiajia Xu, Chao Chen, Yanhua Ye, Yanqiao Ren, Ke Chen, Guofeng Zhou, Chuan Cheng, Yuexiang Peng\",\"doi\":\"10.1177/17562848251360114\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Intrahepatic cholangiocarcinoma (ICC) with obstructive jaundice presents a therapeutic challenge, as most patients are ineligible for surgery. While FOLFOX chemotherapy offers limited survival benefits, drug-eluting bead transarterial chemoembolization (DEB-TACE) combined with percutaneous transhepatic cholangial drainage (PTCD) may improve outcomes by addressing both tumor burden and biliary obstruction.</p><p><strong>Objective: </strong>To evaluate the efficacy and safety of DEB-TACE + PTCD versus DEB-TACE alone in unresectable ICC patients with obstructive jaundice.</p><p><strong>Design: </strong>Retrospective cohort study of 209 patients treated between January 2015 and November 2024.</p><p><strong>Methods: </strong>A total of 209 patients with ICC and obstructive jaundice were included, with 95 patients in the DEB-TACE + PTCD group (D + P group) and 114 patients in the DEB-TACE alone group (DEB group). Tumor responses were evaluated at 3 months to assess treatment efficacy, while statistical analyses of adverse events were conducted to evaluate treatment safety. Kaplan-Meier method was utilized to generate survival curves. Cox analysis was performed to identify factors influencing prognosis.</p><p><strong>Results: </strong>The median progression-free survival and OS were 6 and 14 months in D + P group and 5 and 11 months in the DEB group. The 3-month objective response rate (ORR) and disease control rate (DCR) were 36.2% and 76.6% in the D + P group. While in the DEB group, the ORR and DCR were 34.2% (<i>p</i> = 0.772) and 62.2% (<i>p</i> = 0.026). Multivariate Cox regression analysis revealed that lymph node metastasis (hazard ratio (HR) = 0.727, confidence interval (CI: 0.535-0.987), <i>p</i> = 0.041), level of cancer antigen (CA)-125 (HR = 0.670, CI (0.503-0.894), <i>p</i> = 0.006), and treatment (HR = 1.335, CI (1.002-1.780), <i>p</i> = 0.049) were predictors for prognosis.</p><p><strong>Conclusion: </strong>For patients with unresectable cholangiocarcinoma complicated by obstructive jaundice, DEB-TACE following PTCD may be a safer and more effective treatment.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"18 \",\"pages\":\"17562848251360114\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374100/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848251360114\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251360114","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:肝内胆管癌(ICC)合并梗阻性黄疸是一个治疗挑战,因为大多数患者不适合手术治疗。虽然FOLFOX化疗提供有限的生存益处,但药物洗脱经动脉化疗栓塞(DEB-TACE)联合经皮经肝胆管引流(PTCD)可能通过解决肿瘤负担和胆道梗阻来改善预后。目的:评价DEB-TACE + PTCD与单独DEB-TACE治疗梗阻性黄疸无法切除的ICC患者的疗效和安全性。设计:2015年1月至2024年11月期间接受治疗的209例患者的回顾性队列研究。方法:纳入ICC合并梗阻性黄疸患者209例,其中DEB- tace + PTCD组(D + P组)95例,单独DEB- tace组(DEB组)114例。3个月时评价肿瘤反应,评价治疗效果;对不良事件进行统计分析,评价治疗安全性。采用Kaplan-Meier法生成生存曲线。Cox分析确定影响预后的因素。结果:D + P组的中位无进展生存期和OS分别为6个月和14个月,DEB组的中位无进展生存期和OS分别为5个月和11个月。D + P组3个月客观缓解率(ORR)和疾病控制率(DCR)分别为36.2%和76.6%。而DEB组的ORR和DCR分别为34.2% (p = 0.772)和62.2% (p = 0.026)。多因素Cox回归分析显示,淋巴结转移(危险比(HR) = 0.727,可信区间(CI: 0.535 ~ 0.987), p = 0.041)、癌抗原(CA)-125水平(HR = 0.670, CI (0.503 ~ 0.894), p = 0.006)、治疗(HR = 1.335, CI (1.002 ~ 1.780), p = 0.049)是预后的预测因素。结论:对于不能切除的胆管癌合并梗阻性黄疸患者,PTCD后行DEB-TACE可能是一种更安全有效的治疗方法。
Outcome of adding percutaneous transhepatic cholangial drainage to DEB-TACE in patients with unresectable cholangiocarcinoma with obstructive jaundice: comparison with sole DEB-TACE.
Background: Intrahepatic cholangiocarcinoma (ICC) with obstructive jaundice presents a therapeutic challenge, as most patients are ineligible for surgery. While FOLFOX chemotherapy offers limited survival benefits, drug-eluting bead transarterial chemoembolization (DEB-TACE) combined with percutaneous transhepatic cholangial drainage (PTCD) may improve outcomes by addressing both tumor burden and biliary obstruction.
Objective: To evaluate the efficacy and safety of DEB-TACE + PTCD versus DEB-TACE alone in unresectable ICC patients with obstructive jaundice.
Design: Retrospective cohort study of 209 patients treated between January 2015 and November 2024.
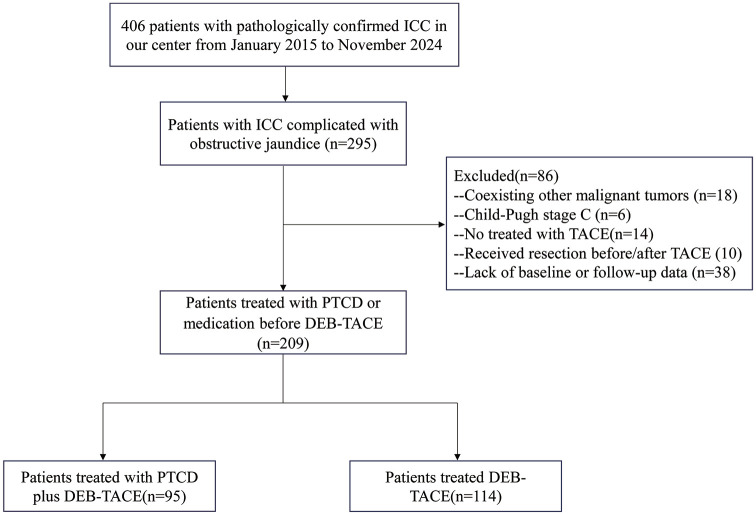
Methods: A total of 209 patients with ICC and obstructive jaundice were included, with 95 patients in the DEB-TACE + PTCD group (D + P group) and 114 patients in the DEB-TACE alone group (DEB group). Tumor responses were evaluated at 3 months to assess treatment efficacy, while statistical analyses of adverse events were conducted to evaluate treatment safety. Kaplan-Meier method was utilized to generate survival curves. Cox analysis was performed to identify factors influencing prognosis.
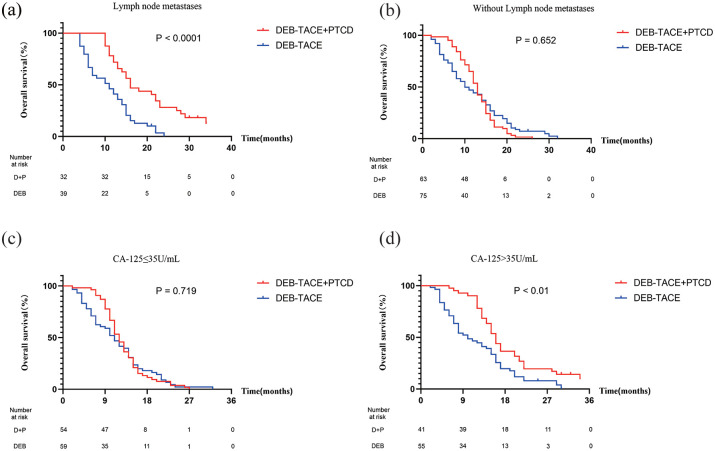
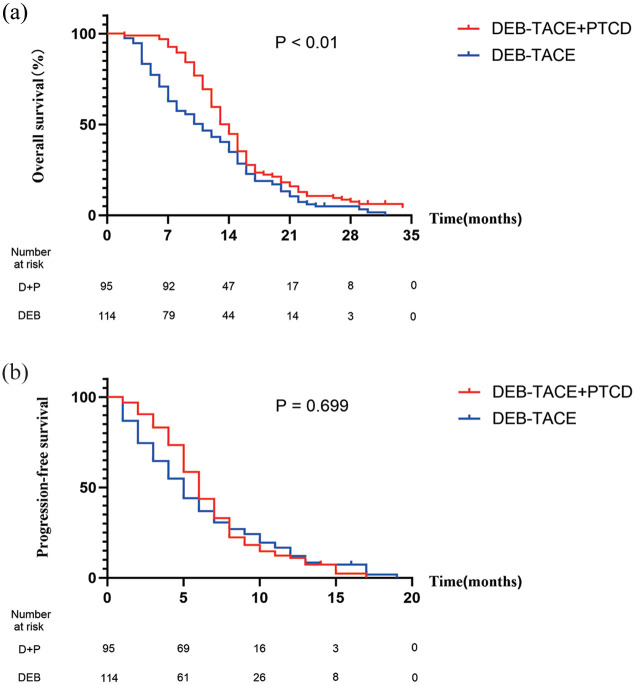
Results: The median progression-free survival and OS were 6 and 14 months in D + P group and 5 and 11 months in the DEB group. The 3-month objective response rate (ORR) and disease control rate (DCR) were 36.2% and 76.6% in the D + P group. While in the DEB group, the ORR and DCR were 34.2% (p = 0.772) and 62.2% (p = 0.026). Multivariate Cox regression analysis revealed that lymph node metastasis (hazard ratio (HR) = 0.727, confidence interval (CI: 0.535-0.987), p = 0.041), level of cancer antigen (CA)-125 (HR = 0.670, CI (0.503-0.894), p = 0.006), and treatment (HR = 1.335, CI (1.002-1.780), p = 0.049) were predictors for prognosis.
Conclusion: For patients with unresectable cholangiocarcinoma complicated by obstructive jaundice, DEB-TACE following PTCD may be a safer and more effective treatment.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


