{"title":"缩短住院医师轮班对患者和医师的影响:系统回顾和荟萃分析。","authors":"Vered Daitch, Itamar Poran, Leonard Leibovici","doi":"10.1186/s13584-025-00715-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prolonged shifts in residency contribute to physician fatigue, cognitive decline, and increased medical errors. This systematic review and meta-analysis evaluate how reducing shift length affects patient-physician safety, physician well-being, and residency training, addressing the ongoing challenge of balancing resident welfare, patient outcomes, and educational standards across varied implementation settings.</p><p><strong>Methods: </strong>A comprehensive search of PubMed, EMBASE, The Cochrane Library, Google Scholar, and opengrey.eu was performed from database inception to January 2024. Eligible studies assessed the effects of duty hour limitations (≤ 24 h) on clinical, educational, or systemic outcomes. Both randomized controlled trials and observational studies were included. Meta-analyses used random-effects models. Risk of bias was assessed with RoB 2.0 and ROBINS-I tools. Subgroup analyses were performed by specialty, shift duration, and publication period. Sensitivity analyses excluded studies with extended timeframes.</p><p><strong>Results: </strong>A total of 108 studies (8 RCTs, 100 observational) were included. Shift shortening was associated with improved resident well-being, including reduced fatigue and work-life balance. Patient safety remained stable, with a significant reduction in 30-day mortality for shifts ≤ 16 h (pooled OR 0.84, 95% CI 0.79-0.89). No significant effect on complications or adverse events was observed. Operative experience showed mixed results, with a non-significant reduction in case volume (pooled std. mean difference 0.65, 95% CI -0.04 to 1.34, P = 0.07), while test scores exhibited minimal changes. Effect directions remained consistent across publication periods. High heterogeneity and risk of bias were observed across most included studies.</p><p><strong>Conclusions: </strong>Shortening shifts to 24 h or less appears to improve residents' satisfaction and work-life balance while maintaining patient safety outcomes. Educational outcomes were mixed; operative experience was preserved in some settings, while effects on non-surgical training remain less clear. These findings underscore the importance of tailoring reforms to specialty needs and training contexts. Future research should examine unstudied outcomes, such as residency attrition or shifts to less demanding specializations, and system-wide implementation costs. A stepped wedge cluster randomized trial is recommended for future policy evaluations.</p><p><strong>Systematic review registration: </strong>PROSPERO CRD42023390197.</p>","PeriodicalId":46694,"journal":{"name":"Israel Journal of Health Policy Research","volume":"14 1","pages":"53"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406601/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of shortening shifts of physicians during their residency on patients and physicians : A systematic review and meta-analysis.\",\"authors\":\"Vered Daitch, Itamar Poran, Leonard Leibovici\",\"doi\":\"10.1186/s13584-025-00715-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prolonged shifts in residency contribute to physician fatigue, cognitive decline, and increased medical errors. This systematic review and meta-analysis evaluate how reducing shift length affects patient-physician safety, physician well-being, and residency training, addressing the ongoing challenge of balancing resident welfare, patient outcomes, and educational standards across varied implementation settings.</p><p><strong>Methods: </strong>A comprehensive search of PubMed, EMBASE, The Cochrane Library, Google Scholar, and opengrey.eu was performed from database inception to January 2024. Eligible studies assessed the effects of duty hour limitations (≤ 24 h) on clinical, educational, or systemic outcomes. Both randomized controlled trials and observational studies were included. Meta-analyses used random-effects models. Risk of bias was assessed with RoB 2.0 and ROBINS-I tools. Subgroup analyses were performed by specialty, shift duration, and publication period. Sensitivity analyses excluded studies with extended timeframes.</p><p><strong>Results: </strong>A total of 108 studies (8 RCTs, 100 observational) were included. Shift shortening was associated with improved resident well-being, including reduced fatigue and work-life balance. Patient safety remained stable, with a significant reduction in 30-day mortality for shifts ≤ 16 h (pooled OR 0.84, 95% CI 0.79-0.89). No significant effect on complications or adverse events was observed. Operative experience showed mixed results, with a non-significant reduction in case volume (pooled std. mean difference 0.65, 95% CI -0.04 to 1.34, P = 0.07), while test scores exhibited minimal changes. Effect directions remained consistent across publication periods. High heterogeneity and risk of bias were observed across most included studies.</p><p><strong>Conclusions: </strong>Shortening shifts to 24 h or less appears to improve residents' satisfaction and work-life balance while maintaining patient safety outcomes. Educational outcomes were mixed; operative experience was preserved in some settings, while effects on non-surgical training remain less clear. These findings underscore the importance of tailoring reforms to specialty needs and training contexts. Future research should examine unstudied outcomes, such as residency attrition or shifts to less demanding specializations, and system-wide implementation costs. A stepped wedge cluster randomized trial is recommended for future policy evaluations.</p><p><strong>Systematic review registration: </strong>PROSPERO CRD42023390197.</p>\",\"PeriodicalId\":46694,\"journal\":{\"name\":\"Israel Journal of Health Policy Research\",\"volume\":\"14 1\",\"pages\":\"53\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406601/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Israel Journal of Health Policy Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13584-025-00715-2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Israel Journal of Health Policy Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13584-025-00715-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
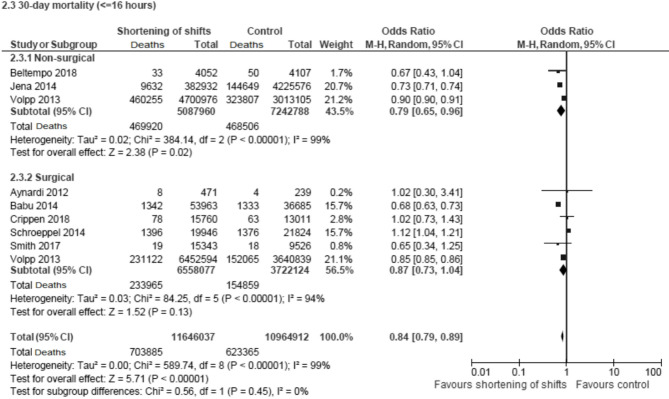
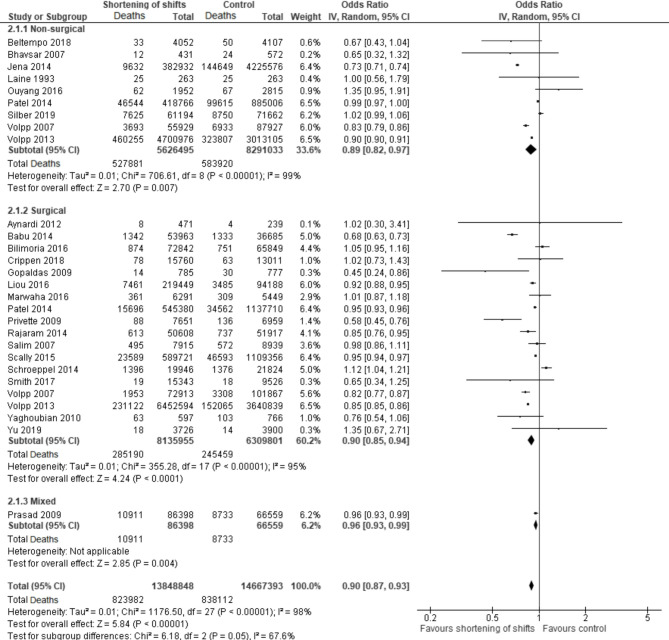
背景:住院医师长时间轮班会导致医生疲劳、认知能力下降和医疗差错增加。本系统综述和荟萃分析评估了减少轮班长度如何影响患者-医生安全、医生福祉和住院医师培训,解决了在不同实施环境中平衡住院医师福利、患者预后和教育标准的持续挑战。方法:综合检索PubMed、EMBASE、Cochrane Library、谷歌Scholar和opengrey。eu从数据库建立到2024年1月执行。符合条件的研究评估了值班时间限制(≤24小时)对临床、教育或系统结果的影响。包括随机对照试验和观察性研究。荟萃分析使用随机效应模型。采用rob2.0和ROBINS-I工具评估偏倚风险。亚组分析按专业、轮班时间和出版期进行。敏感性分析排除了时间范围较长的研究。结果:共纳入108项研究(8项随机对照试验,100项观察性研究)。轮班缩短与居民幸福感的提高有关,包括减少疲劳和工作与生活的平衡。患者安全性保持稳定,轮班≤16小时的30天死亡率显著降低(合并OR 0.84, 95% CI 0.79-0.89)。未观察到并发症或不良事件的显著影响。手术经验显示混合结果,病例量无显著减少(合并std平均差异0.65,95% CI -0.04至1.34,P = 0.07),而测试分数变化最小。影响方向在整个出版期间保持一致。在大多数纳入的研究中观察到高异质性和偏倚风险。结论:缩短轮班至24小时或更短的时间可以提高住院医生的满意度和工作与生活的平衡,同时保持患者的安全结果。教育成果好坏参半;在某些情况下保留了手术经验,而对非手术培训的影响尚不清楚。这些发现强调了根据专业需求和培训环境进行调整改革的重要性。未来的研究应检查未研究的结果,如住院医师流失或转移到要求较低的专业,以及全系统的实施成本。建议在未来的政策评估中采用楔形阶梯聚类随机试验。系统评价注册:PROSPERO CRD42023390197。
The impact of shortening shifts of physicians during their residency on patients and physicians : A systematic review and meta-analysis.
Background: Prolonged shifts in residency contribute to physician fatigue, cognitive decline, and increased medical errors. This systematic review and meta-analysis evaluate how reducing shift length affects patient-physician safety, physician well-being, and residency training, addressing the ongoing challenge of balancing resident welfare, patient outcomes, and educational standards across varied implementation settings.
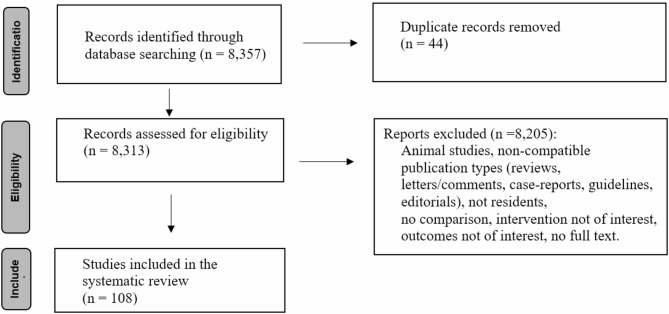
Methods: A comprehensive search of PubMed, EMBASE, The Cochrane Library, Google Scholar, and opengrey.eu was performed from database inception to January 2024. Eligible studies assessed the effects of duty hour limitations (≤ 24 h) on clinical, educational, or systemic outcomes. Both randomized controlled trials and observational studies were included. Meta-analyses used random-effects models. Risk of bias was assessed with RoB 2.0 and ROBINS-I tools. Subgroup analyses were performed by specialty, shift duration, and publication period. Sensitivity analyses excluded studies with extended timeframes.
Results: A total of 108 studies (8 RCTs, 100 observational) were included. Shift shortening was associated with improved resident well-being, including reduced fatigue and work-life balance. Patient safety remained stable, with a significant reduction in 30-day mortality for shifts ≤ 16 h (pooled OR 0.84, 95% CI 0.79-0.89). No significant effect on complications or adverse events was observed. Operative experience showed mixed results, with a non-significant reduction in case volume (pooled std. mean difference 0.65, 95% CI -0.04 to 1.34, P = 0.07), while test scores exhibited minimal changes. Effect directions remained consistent across publication periods. High heterogeneity and risk of bias were observed across most included studies.
Conclusions: Shortening shifts to 24 h or less appears to improve residents' satisfaction and work-life balance while maintaining patient safety outcomes. Educational outcomes were mixed; operative experience was preserved in some settings, while effects on non-surgical training remain less clear. These findings underscore the importance of tailoring reforms to specialty needs and training contexts. Future research should examine unstudied outcomes, such as residency attrition or shifts to less demanding specializations, and system-wide implementation costs. A stepped wedge cluster randomized trial is recommended for future policy evaluations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


