{"title":"静脉动脉ECMO患者的生存预测因素和临床结果:一项7年回顾性研究。","authors":"Thavat Chanchayanon, Mantana Saetang, Sutthiphat Wangpholpattanasiri, Ratikorn Boonchai, Pongsanae Duangpakdee","doi":"10.1155/ccrp/5588093","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose:</b> Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a life-saving intervention for refractory cardiopulmonary failure. Identifying factors associated with survival is essential for optimizing patient selection and management. In this study, we aimed to identify VA-ECMO survival predictors and evaluate the associated complications, costs, and outcomes. <b>Methods:</b> A retrospective analysis was conducted on data from 123 adult patients who underwent VA-ECMO at the Songklanagarind Hospital between 2017 and 2023. Clinical characteristics, ECMO-related complications, hospital expenses, and survival outcomes were analyzed. Univariate and multivariate logistic regression analyses were used to determine independent predictors of survival. <b>Results:</b> Fifty (40.7%) patients survived until hospital discharge. Compared to central VA-ECMO, peripheral VA-ECMO was significantly associated with improved survival (adjusted OR: 26.44, 95% CI: 1.95-358.7, <i>p</i> = 0.014). Preexisting liver dysfunction (adjusted OR: 0.27, 95% CI: 0.09-0.79, <i>p</i> = 0.016) and renal dysfunction (adjusted OR: 0.29, 95% CI: 0.1-0.85, <i>p</i> = 0.023) were independent mortality predictors. Survival odds were significantly lower in patients with American Society of Anesthesiologists (ASA) Class 5 (adjusted OR: 0.07, 95% CI: 0.01-0.67, <i>p</i> = 0.022). Neurological complications were more common in nonsurvivors than in survivors (41.1% vs. 18%, <i>p</i> = 0.012). Survivors had significantly higher total hospital costs (997,563.5 vs. 696,191 THB, <i>p</i> = 0.004) and longer hospital stays (28.5 vs. 3 days, <i>p</i> < 0.001). The multivariate model demonstrated strong predictive performance, with an area under the curve of 0.85. <b>Conclusions:</b> ECMO cannulation strategy, preexisting liver and renal dysfunction, and ASA classification were key factors associated with survival. Peripheral VA-ECMO was associated with better outcomes, and organ dysfunction significantly increased the mortality risk.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2025 ","pages":"5588093"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396898/pdf/","citationCount":"0","resultStr":"{\"title\":\"Survival Predictors and Clinical Outcomes in Patients Undergoing Venoarterial ECMO: A 7-Year Retrospective Study.\",\"authors\":\"Thavat Chanchayanon, Mantana Saetang, Sutthiphat Wangpholpattanasiri, Ratikorn Boonchai, Pongsanae Duangpakdee\",\"doi\":\"10.1155/ccrp/5588093\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Purpose:</b> Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a life-saving intervention for refractory cardiopulmonary failure. Identifying factors associated with survival is essential for optimizing patient selection and management. In this study, we aimed to identify VA-ECMO survival predictors and evaluate the associated complications, costs, and outcomes. <b>Methods:</b> A retrospective analysis was conducted on data from 123 adult patients who underwent VA-ECMO at the Songklanagarind Hospital between 2017 and 2023. Clinical characteristics, ECMO-related complications, hospital expenses, and survival outcomes were analyzed. Univariate and multivariate logistic regression analyses were used to determine independent predictors of survival. <b>Results:</b> Fifty (40.7%) patients survived until hospital discharge. Compared to central VA-ECMO, peripheral VA-ECMO was significantly associated with improved survival (adjusted OR: 26.44, 95% CI: 1.95-358.7, <i>p</i> = 0.014). Preexisting liver dysfunction (adjusted OR: 0.27, 95% CI: 0.09-0.79, <i>p</i> = 0.016) and renal dysfunction (adjusted OR: 0.29, 95% CI: 0.1-0.85, <i>p</i> = 0.023) were independent mortality predictors. Survival odds were significantly lower in patients with American Society of Anesthesiologists (ASA) Class 5 (adjusted OR: 0.07, 95% CI: 0.01-0.67, <i>p</i> = 0.022). Neurological complications were more common in nonsurvivors than in survivors (41.1% vs. 18%, <i>p</i> = 0.012). Survivors had significantly higher total hospital costs (997,563.5 vs. 696,191 THB, <i>p</i> = 0.004) and longer hospital stays (28.5 vs. 3 days, <i>p</i> < 0.001). The multivariate model demonstrated strong predictive performance, with an area under the curve of 0.85. <b>Conclusions:</b> ECMO cannulation strategy, preexisting liver and renal dysfunction, and ASA classification were key factors associated with survival. Peripheral VA-ECMO was associated with better outcomes, and organ dysfunction significantly increased the mortality risk.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2025 \",\"pages\":\"5588093\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396898/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/ccrp/5588093\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/5588093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
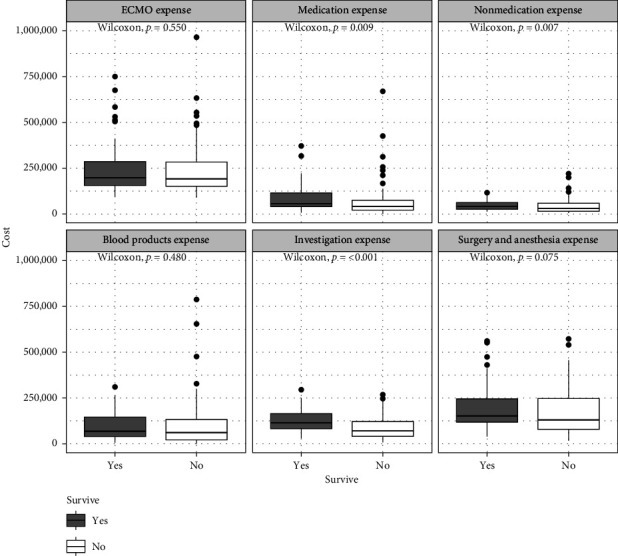
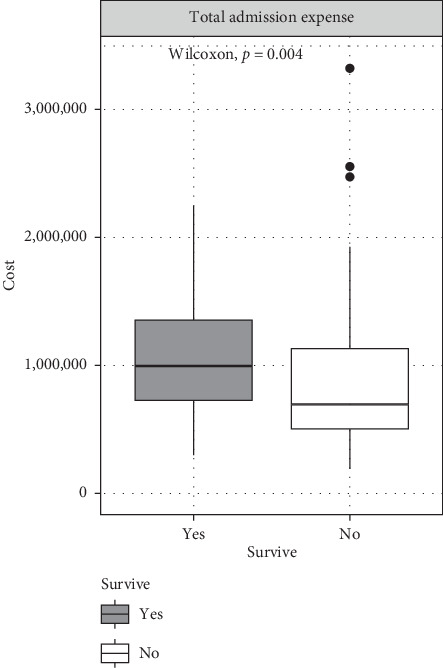
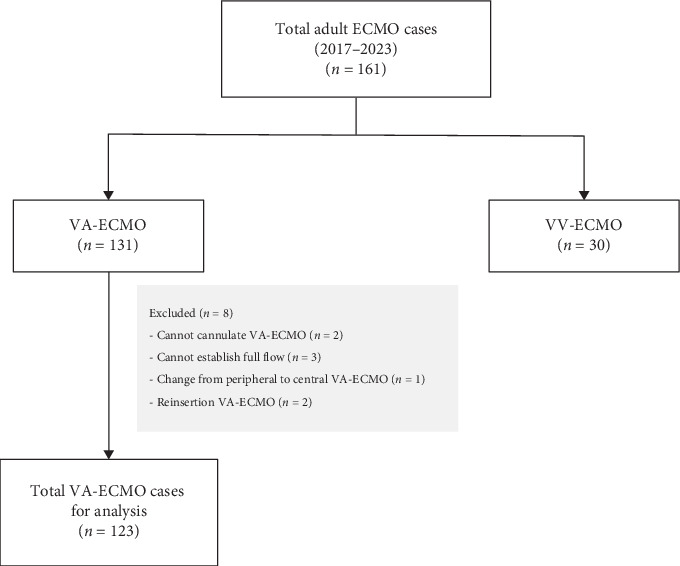
目的:静脉体外膜氧合(VA-ECMO)是一种挽救难治性心肺衰竭生命的干预措施。确定与生存相关的因素对于优化患者选择和管理至关重要。在这项研究中,我们旨在确定VA-ECMO的生存预测因素,并评估相关的并发症、成本和结果。方法:回顾性分析2017年至2023年在Songklanagarind医院接受VA-ECMO治疗的123例成年患者的数据。分析临床特征、ecmo相关并发症、住院费用和生存结果。采用单因素和多因素logistic回归分析确定独立的生存预测因子。结果:50例(40.7%)患者存活至出院。与中心VA-ECMO相比,外周VA-ECMO与生存率的提高显著相关(调整OR: 26.44, 95% CI: 1.95-358.7, p = 0.014)。先前存在的肝功能障碍(校正OR: 0.27, 95% CI: 0.09-0.79, p = 0.016)和肾功能障碍(校正OR: 0.29, 95% CI: 0.1-0.85, p = 0.023)是独立的死亡率预测因子。美国麻醉医师学会(ASA) 5级患者的生存几率明显较低(校正OR: 0.07, 95% CI: 0.01-0.67, p = 0.022)。神经系统并发症在非幸存者中比在幸存者中更常见(41.1%比18%,p = 0.012)。幸存者的总住院费用明显较高(997,563.5比696,191 THB, p = 0.004),住院时间较长(28.5比3天,p < 0.001)。多元模型具有较强的预测能力,曲线下面积为0.85。结论:ECMO插管策略、既往存在的肝肾功能障碍和ASA分级是影响生存率的关键因素。外周VA-ECMO与更好的预后相关,器官功能障碍显著增加死亡风险。
Survival Predictors and Clinical Outcomes in Patients Undergoing Venoarterial ECMO: A 7-Year Retrospective Study.
Purpose: Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a life-saving intervention for refractory cardiopulmonary failure. Identifying factors associated with survival is essential for optimizing patient selection and management. In this study, we aimed to identify VA-ECMO survival predictors and evaluate the associated complications, costs, and outcomes. Methods: A retrospective analysis was conducted on data from 123 adult patients who underwent VA-ECMO at the Songklanagarind Hospital between 2017 and 2023. Clinical characteristics, ECMO-related complications, hospital expenses, and survival outcomes were analyzed. Univariate and multivariate logistic regression analyses were used to determine independent predictors of survival. Results: Fifty (40.7%) patients survived until hospital discharge. Compared to central VA-ECMO, peripheral VA-ECMO was significantly associated with improved survival (adjusted OR: 26.44, 95% CI: 1.95-358.7, p = 0.014). Preexisting liver dysfunction (adjusted OR: 0.27, 95% CI: 0.09-0.79, p = 0.016) and renal dysfunction (adjusted OR: 0.29, 95% CI: 0.1-0.85, p = 0.023) were independent mortality predictors. Survival odds were significantly lower in patients with American Society of Anesthesiologists (ASA) Class 5 (adjusted OR: 0.07, 95% CI: 0.01-0.67, p = 0.022). Neurological complications were more common in nonsurvivors than in survivors (41.1% vs. 18%, p = 0.012). Survivors had significantly higher total hospital costs (997,563.5 vs. 696,191 THB, p = 0.004) and longer hospital stays (28.5 vs. 3 days, p < 0.001). The multivariate model demonstrated strong predictive performance, with an area under the curve of 0.85. Conclusions: ECMO cannulation strategy, preexisting liver and renal dysfunction, and ASA classification were key factors associated with survival. Peripheral VA-ECMO was associated with better outcomes, and organ dysfunction significantly increased the mortality risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


