{"title":"院外心脏骤停后昏迷患者的呼吸驱动与生存","authors":"Purich Sintrirat, Veerapong Vattanavanit","doi":"10.2147/OAEM.S511715","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to explore alterations in respiratory drive in comatose patients after out-of-hospital cardiac arrest (OHCA) and their association with survival outcomes.</p><p><strong>Patients and methods: </strong>A prospective cohort study was conducted on comatose patients with OHCA who were admitted between October 2022 and October 2024. Patients were followed until their discharge from the hospital and subsequently categorized into survivors and non-survivors. Respiratory drive was evaluated using P0.1, representing the airway occlusion pressure measured within the first 100 ms of inspiration, as displayed on the ventilator. Measurements were collected together with additional parameters at 24, 48, and 72 h following admission.</p><p><strong>Results: </strong>The analysis involved 30 patients, with an in-hospital mortality rate of 53.3%. Over the 72-h observation period, P0.1 values were greater in survivors than in non-survivors; however, this difference was not statistically significant. During the first 24 h, survivors demonstrated significantly lower tidal volumes per predicted body weight (P = 0.034). P0.1 values ranging from 1.5 to 3.5 cmH<sub>2</sub>O in the initial 24 h were independently associated with reduced in-hospital mortality (adjusted OR 0.043, 95% CI 0.003-0.588, P = 0.018).</p><p><strong>Conclusion: </strong>A trend toward elevated P0.1 levels in survivors was observed. P0.1 values within the range of 1.5-3.5 cmH<sub>2</sub>O during the first 24 h were linked to a lower mortality rate. These results indicate that P0.1 could be utilized as a prognostic indicator for comatose patients following OHCA.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"233-245"},"PeriodicalIF":1.5000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377396/pdf/","citationCount":"0","resultStr":"{\"title\":\"Respiratory Drive and Survival in Comatose Out-of-Hospital Post-Cardiac Arrest Patients.\",\"authors\":\"Purich Sintrirat, Veerapong Vattanavanit\",\"doi\":\"10.2147/OAEM.S511715\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to explore alterations in respiratory drive in comatose patients after out-of-hospital cardiac arrest (OHCA) and their association with survival outcomes.</p><p><strong>Patients and methods: </strong>A prospective cohort study was conducted on comatose patients with OHCA who were admitted between October 2022 and October 2024. Patients were followed until their discharge from the hospital and subsequently categorized into survivors and non-survivors. Respiratory drive was evaluated using P0.1, representing the airway occlusion pressure measured within the first 100 ms of inspiration, as displayed on the ventilator. Measurements were collected together with additional parameters at 24, 48, and 72 h following admission.</p><p><strong>Results: </strong>The analysis involved 30 patients, with an in-hospital mortality rate of 53.3%. Over the 72-h observation period, P0.1 values were greater in survivors than in non-survivors; however, this difference was not statistically significant. During the first 24 h, survivors demonstrated significantly lower tidal volumes per predicted body weight (P = 0.034). P0.1 values ranging from 1.5 to 3.5 cmH<sub>2</sub>O in the initial 24 h were independently associated with reduced in-hospital mortality (adjusted OR 0.043, 95% CI 0.003-0.588, P = 0.018).</p><p><strong>Conclusion: </strong>A trend toward elevated P0.1 levels in survivors was observed. P0.1 values within the range of 1.5-3.5 cmH<sub>2</sub>O during the first 24 h were linked to a lower mortality rate. These results indicate that P0.1 could be utilized as a prognostic indicator for comatose patients following OHCA.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"17 \",\"pages\":\"233-245\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377396/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S511715\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S511715","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Respiratory Drive and Survival in Comatose Out-of-Hospital Post-Cardiac Arrest Patients.
Purpose: This study aimed to explore alterations in respiratory drive in comatose patients after out-of-hospital cardiac arrest (OHCA) and their association with survival outcomes.
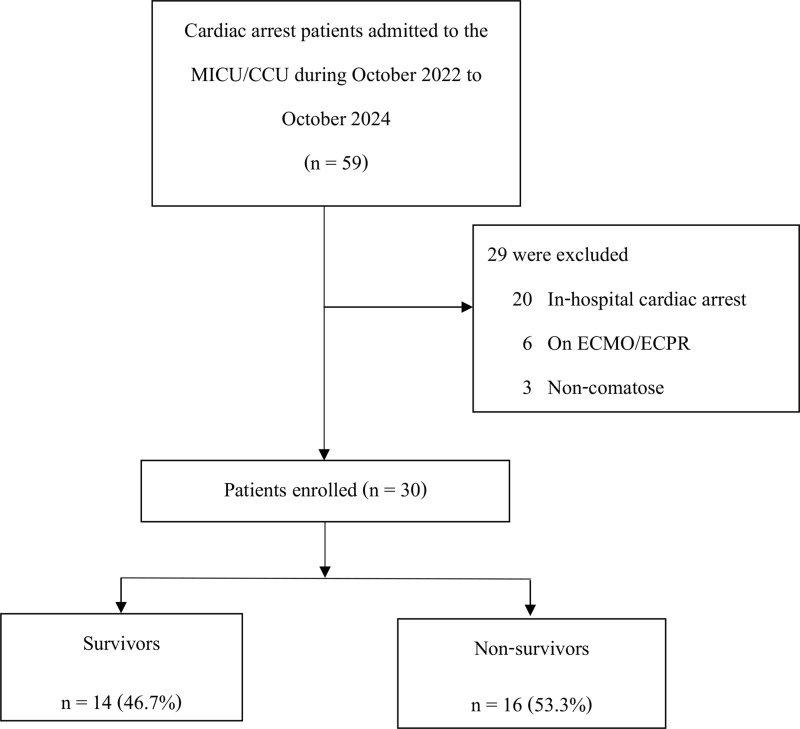
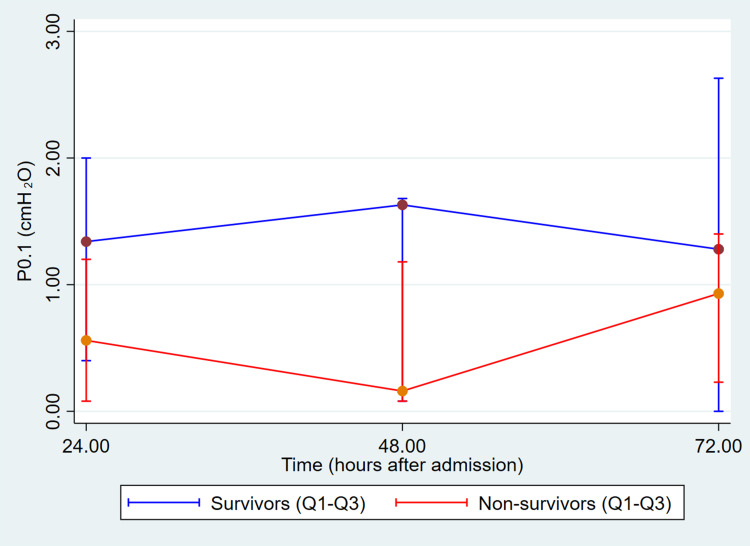
Patients and methods: A prospective cohort study was conducted on comatose patients with OHCA who were admitted between October 2022 and October 2024. Patients were followed until their discharge from the hospital and subsequently categorized into survivors and non-survivors. Respiratory drive was evaluated using P0.1, representing the airway occlusion pressure measured within the first 100 ms of inspiration, as displayed on the ventilator. Measurements were collected together with additional parameters at 24, 48, and 72 h following admission.
Results: The analysis involved 30 patients, with an in-hospital mortality rate of 53.3%. Over the 72-h observation period, P0.1 values were greater in survivors than in non-survivors; however, this difference was not statistically significant. During the first 24 h, survivors demonstrated significantly lower tidal volumes per predicted body weight (P = 0.034). P0.1 values ranging from 1.5 to 3.5 cmH2O in the initial 24 h were independently associated with reduced in-hospital mortality (adjusted OR 0.043, 95% CI 0.003-0.588, P = 0.018).
Conclusion: A trend toward elevated P0.1 levels in survivors was observed. P0.1 values within the range of 1.5-3.5 cmH2O during the first 24 h were linked to a lower mortality rate. These results indicate that P0.1 could be utilized as a prognostic indicator for comatose patients following OHCA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


