Antonio Malvasi, Lorenzo E Malgieri, Michael Stark, Edoardo Di Naro, Dan Farine, Giorgio Maria Baldini, Miriam Dellino, Murat Yassa, Andrea Tinelli, Antonella Vimercati, Tommaso Difonzo
{"title":"人工智能难产算法(AIDA)对Robson分类组剖宫产术的贡献。","authors":"Antonio Malvasi, Lorenzo E Malgieri, Michael Stark, Edoardo Di Naro, Dan Farine, Giorgio Maria Baldini, Miriam Dellino, Murat Yassa, Andrea Tinelli, Antonella Vimercati, Tommaso Difonzo","doi":"10.3390/jimaging11080276","DOIUrl":null,"url":null,"abstract":"<p><p>Global cesarean section (CS) rates continue to rise, with the Robson classification widely used for analysis. However, Robson Group 2A patients (nulliparous women with induced labor) show disproportionately high CS rates that cannot be fully explained by demographic factors alone. This study explored how the Artificial Intelligence Dystocia Algorithm (AIDA) could enhance the Robson system by providing detailed information on geometric dystocia, thereby facilitating better understanding of factors contributing to CS and developing more targeted reduction strategies. The authors conducted a comprehensive literature review analyzing both classification systems across multiple databases and developed a theoretical framework for integration. AIDA categorized labor cases into five classes (0-4) by analyzing four key geometric parameters measured through intrapartum ultrasound: angle of progression (AoP), asynclitism degree (AD), head-symphysis distance (HSD), and midline angle (MLA). Significant asynclitism (AD ≥ 7.0 mm) was strongly associated with CS regardless of other parameters, potentially explaining many \"failure to progress\" cases in Robson Group 2A patients. The proposed integration created a combined classification providing both population-level and individual geometric risk assessment. The integration of AIDA with the Robson classification represented a potentially valuable advancement in CS risk assessment, combining population-level stratification with individual-level geometric assessment to enable more personalized obstetric care. Future validation studies across diverse settings are needed to establish clinical utility.</p>","PeriodicalId":37035,"journal":{"name":"Journal of Imaging","volume":"11 8","pages":""},"PeriodicalIF":2.7000,"publicationDate":"2025-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387988/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Contribution of AIDA (Artificial Intelligence Dystocia Algorithm) to Cesarean Section Within Robson Classification Group.\",\"authors\":\"Antonio Malvasi, Lorenzo E Malgieri, Michael Stark, Edoardo Di Naro, Dan Farine, Giorgio Maria Baldini, Miriam Dellino, Murat Yassa, Andrea Tinelli, Antonella Vimercati, Tommaso Difonzo\",\"doi\":\"10.3390/jimaging11080276\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Global cesarean section (CS) rates continue to rise, with the Robson classification widely used for analysis. However, Robson Group 2A patients (nulliparous women with induced labor) show disproportionately high CS rates that cannot be fully explained by demographic factors alone. This study explored how the Artificial Intelligence Dystocia Algorithm (AIDA) could enhance the Robson system by providing detailed information on geometric dystocia, thereby facilitating better understanding of factors contributing to CS and developing more targeted reduction strategies. The authors conducted a comprehensive literature review analyzing both classification systems across multiple databases and developed a theoretical framework for integration. AIDA categorized labor cases into five classes (0-4) by analyzing four key geometric parameters measured through intrapartum ultrasound: angle of progression (AoP), asynclitism degree (AD), head-symphysis distance (HSD), and midline angle (MLA). Significant asynclitism (AD ≥ 7.0 mm) was strongly associated with CS regardless of other parameters, potentially explaining many \\\"failure to progress\\\" cases in Robson Group 2A patients. The proposed integration created a combined classification providing both population-level and individual geometric risk assessment. The integration of AIDA with the Robson classification represented a potentially valuable advancement in CS risk assessment, combining population-level stratification with individual-level geometric assessment to enable more personalized obstetric care. Future validation studies across diverse settings are needed to establish clinical utility.</p>\",\"PeriodicalId\":37035,\"journal\":{\"name\":\"Journal of Imaging\",\"volume\":\"11 8\",\"pages\":\"\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-08-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387988/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Imaging\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/jimaging11080276\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMAGING SCIENCE & PHOTOGRAPHIC TECHNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/jimaging11080276","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMAGING SCIENCE & PHOTOGRAPHIC TECHNOLOGY","Score":null,"Total":0}
The Contribution of AIDA (Artificial Intelligence Dystocia Algorithm) to Cesarean Section Within Robson Classification Group.
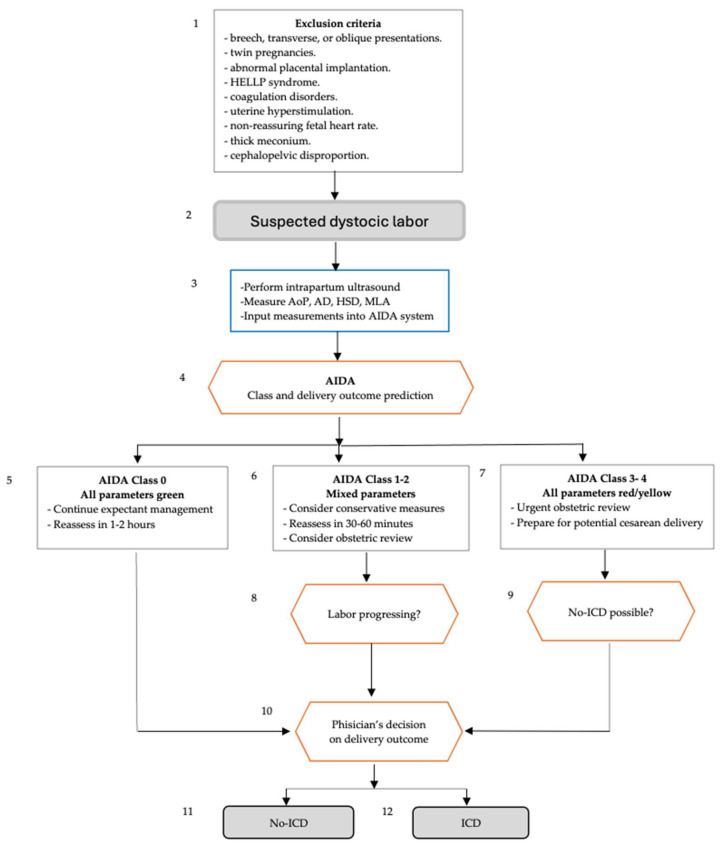
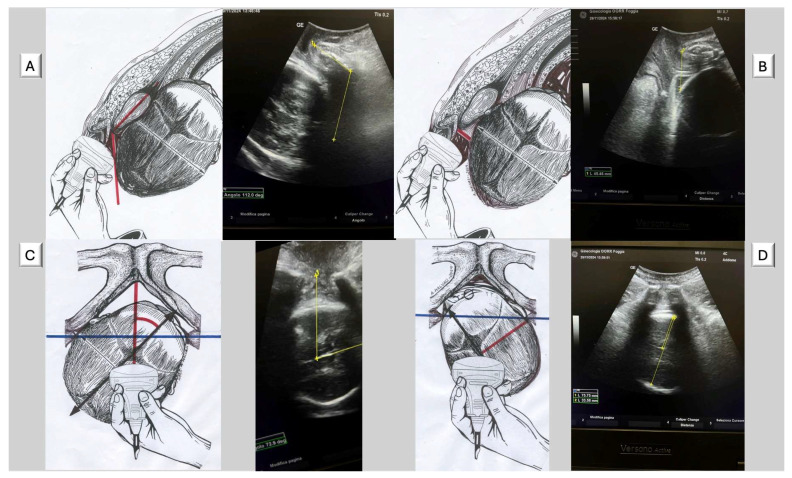
Global cesarean section (CS) rates continue to rise, with the Robson classification widely used for analysis. However, Robson Group 2A patients (nulliparous women with induced labor) show disproportionately high CS rates that cannot be fully explained by demographic factors alone. This study explored how the Artificial Intelligence Dystocia Algorithm (AIDA) could enhance the Robson system by providing detailed information on geometric dystocia, thereby facilitating better understanding of factors contributing to CS and developing more targeted reduction strategies. The authors conducted a comprehensive literature review analyzing both classification systems across multiple databases and developed a theoretical framework for integration. AIDA categorized labor cases into five classes (0-4) by analyzing four key geometric parameters measured through intrapartum ultrasound: angle of progression (AoP), asynclitism degree (AD), head-symphysis distance (HSD), and midline angle (MLA). Significant asynclitism (AD ≥ 7.0 mm) was strongly associated with CS regardless of other parameters, potentially explaining many "failure to progress" cases in Robson Group 2A patients. The proposed integration created a combined classification providing both population-level and individual geometric risk assessment. The integration of AIDA with the Robson classification represented a potentially valuable advancement in CS risk assessment, combining population-level stratification with individual-level geometric assessment to enable more personalized obstetric care. Future validation studies across diverse settings are needed to establish clinical utility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


