Jaeoh Lee, Sripal Bangalore, Kyeong Ho Yun, Sang-Hyup Lee, Yong-Joon Lee, Seung-Jun Lee, Sung-Jin Hong, Chul-Min Ahn, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Donghoon Choi, Yangsoo Jang, Bum-Kee Hong, Myeong-Ki Hong
{"title":"LDL-C变异性的预后意义及其与降脂策略的关联:来自RACING和LODESTAR试验的见解","authors":"Jaeoh Lee, Sripal Bangalore, Kyeong Ho Yun, Sang-Hyup Lee, Yong-Joon Lee, Seung-Jun Lee, Sung-Jin Hong, Chul-Min Ahn, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Donghoon Choi, Yangsoo Jang, Bum-Kee Hong, Myeong-Ki Hong","doi":"10.3349/ymj.2024.0476","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We aimed to compare the visit-to-visit variability in low-density lipoprotein cholesterol (LDL-C) according to different lipid-lowering strategies and evaluate its prognostic implications using data from previous trials.</p><p><strong>Materials and methods: </strong>We analyzed two randomized clinical trials: the RACING trial and the LODESTAR trial. LDL-C variability was evaluated using standard deviation (SD), coefficient of variation, and variation independent of mean. The primary endpoint was a composite of death, myocardial infarction, stroke, or coronary revascularization.</p><p><strong>Results: </strong>Among the 6800 patients included, when compared with patients randomized to high-intensity statins, LDL-C variability was similar in the group randomized to moderate-intensity statin plus ezetimibe combination, but it was higher in those randomized to treat-to-target strategy. The variability in LDL-C (by SD) was a predictor of primary endpoint even after adjustment for lipid-lowering strategy and mean LDL-C (hazard ratio 1.024; 95% confidence interval 1.014 to 1.035; <i>p</i><0.001). Every 1-SD increase in LDL-C variability (SD) was also independently associated with higher risk of myocardial infarction by 2.1%, stroke by 3.5%, and coronary revascularization by 2.7%.</p><p><strong>Conclusion: </strong>Compared to high-intensity statin therapy, LDL-C variability was not increased with the moderate-intensity statin plus ezetimibe combination therapy; however, it was increased in the treat-to-target strategy. Even among those treated with moderate- or high-intensity statins or statins with a target LDL-C levels of 50-70 mg/dL, increased LDL-C variability was associated with higher risk of adverse cardiovascular outcomes.</p>","PeriodicalId":23765,"journal":{"name":"Yonsei Medical Journal","volume":"66 9","pages":"537-544"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394753/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic Implication of LDL-C Variability and Its Association with Lipid-Lowering Strategies: Insights from the RACING and LODESTAR Trials.\",\"authors\":\"Jaeoh Lee, Sripal Bangalore, Kyeong Ho Yun, Sang-Hyup Lee, Yong-Joon Lee, Seung-Jun Lee, Sung-Jin Hong, Chul-Min Ahn, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Donghoon Choi, Yangsoo Jang, Bum-Kee Hong, Myeong-Ki Hong\",\"doi\":\"10.3349/ymj.2024.0476\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We aimed to compare the visit-to-visit variability in low-density lipoprotein cholesterol (LDL-C) according to different lipid-lowering strategies and evaluate its prognostic implications using data from previous trials.</p><p><strong>Materials and methods: </strong>We analyzed two randomized clinical trials: the RACING trial and the LODESTAR trial. LDL-C variability was evaluated using standard deviation (SD), coefficient of variation, and variation independent of mean. The primary endpoint was a composite of death, myocardial infarction, stroke, or coronary revascularization.</p><p><strong>Results: </strong>Among the 6800 patients included, when compared with patients randomized to high-intensity statins, LDL-C variability was similar in the group randomized to moderate-intensity statin plus ezetimibe combination, but it was higher in those randomized to treat-to-target strategy. The variability in LDL-C (by SD) was a predictor of primary endpoint even after adjustment for lipid-lowering strategy and mean LDL-C (hazard ratio 1.024; 95% confidence interval 1.014 to 1.035; <i>p</i><0.001). Every 1-SD increase in LDL-C variability (SD) was also independently associated with higher risk of myocardial infarction by 2.1%, stroke by 3.5%, and coronary revascularization by 2.7%.</p><p><strong>Conclusion: </strong>Compared to high-intensity statin therapy, LDL-C variability was not increased with the moderate-intensity statin plus ezetimibe combination therapy; however, it was increased in the treat-to-target strategy. Even among those treated with moderate- or high-intensity statins or statins with a target LDL-C levels of 50-70 mg/dL, increased LDL-C variability was associated with higher risk of adverse cardiovascular outcomes.</p>\",\"PeriodicalId\":23765,\"journal\":{\"name\":\"Yonsei Medical Journal\",\"volume\":\"66 9\",\"pages\":\"537-544\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394753/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Yonsei Medical Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3349/ymj.2024.0476\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Yonsei Medical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3349/ymj.2024.0476","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
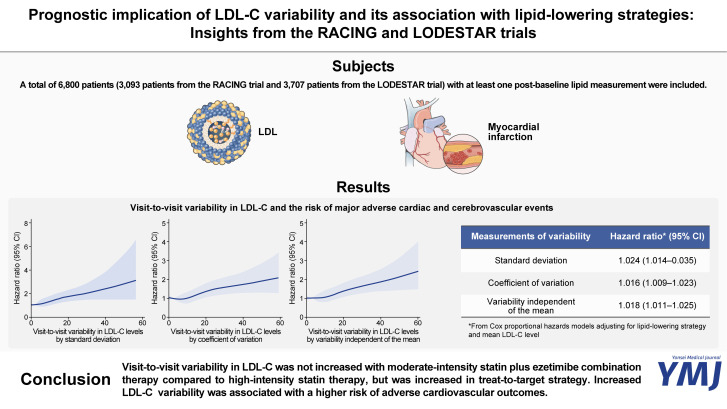
Prognostic Implication of LDL-C Variability and Its Association with Lipid-Lowering Strategies: Insights from the RACING and LODESTAR Trials.
Purpose: We aimed to compare the visit-to-visit variability in low-density lipoprotein cholesterol (LDL-C) according to different lipid-lowering strategies and evaluate its prognostic implications using data from previous trials.
Materials and methods: We analyzed two randomized clinical trials: the RACING trial and the LODESTAR trial. LDL-C variability was evaluated using standard deviation (SD), coefficient of variation, and variation independent of mean. The primary endpoint was a composite of death, myocardial infarction, stroke, or coronary revascularization.
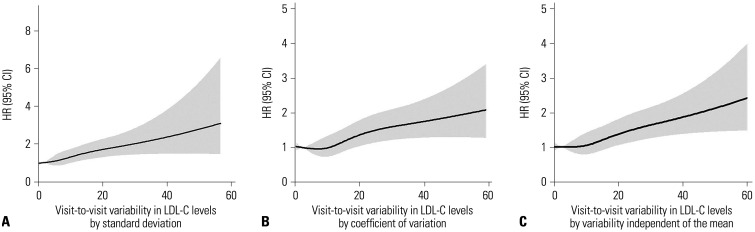
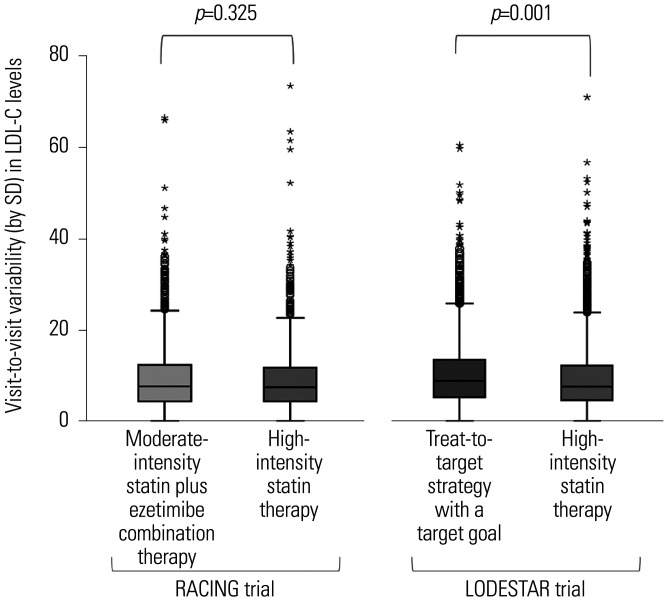
Results: Among the 6800 patients included, when compared with patients randomized to high-intensity statins, LDL-C variability was similar in the group randomized to moderate-intensity statin plus ezetimibe combination, but it was higher in those randomized to treat-to-target strategy. The variability in LDL-C (by SD) was a predictor of primary endpoint even after adjustment for lipid-lowering strategy and mean LDL-C (hazard ratio 1.024; 95% confidence interval 1.014 to 1.035; p<0.001). Every 1-SD increase in LDL-C variability (SD) was also independently associated with higher risk of myocardial infarction by 2.1%, stroke by 3.5%, and coronary revascularization by 2.7%.
Conclusion: Compared to high-intensity statin therapy, LDL-C variability was not increased with the moderate-intensity statin plus ezetimibe combination therapy; however, it was increased in the treat-to-target strategy. Even among those treated with moderate- or high-intensity statins or statins with a target LDL-C levels of 50-70 mg/dL, increased LDL-C variability was associated with higher risk of adverse cardiovascular outcomes.
期刊介绍:
The goal of the Yonsei Medical Journal (YMJ) is to publish high quality manuscripts dedicated to clinical or basic research. Any authors affiliated with an accredited biomedical institution may submit manuscripts of original articles, review articles, case reports, brief communications, and letters to the Editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


