Carl Grabitz, Nima Memaran, Rizky I Sugianto, Jeanine von der Born, Mila Bukova, Elena Lehmann, Ann-Kathrin Konuhov, Dennis Holzwart, Anika Großhennig, Elke Wühl, Bernhard M W Schmidt, Anette Melk
{"title":"停止高血压和改善肾移植后儿童生活(SOPHOCLES):一项随机对照多中心试验的研究方案。","authors":"Carl Grabitz, Nima Memaran, Rizky I Sugianto, Jeanine von der Born, Mila Bukova, Elena Lehmann, Ann-Kathrin Konuhov, Dennis Holzwart, Anika Großhennig, Elke Wühl, Bernhard M W Schmidt, Anette Melk","doi":"10.1186/s13063-025-09033-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular disease is a major morbidity in children after kidney transplantation, limiting life expectancy and impairing graft function. Arterial hypertension is the dominant cardiovascular risk factor and highly abundant in this patient group. Arterial hypertension can cause left ventricular hypertrophy, which is predictive of cardiovascular death. Left ventricular hypertrophy can be non-invasively assessed by measuring left ventricular mass. Observational data indicated that intensified blood pressure control was associated with a significant reduction of left ventricular mass. Based on evidence from the randomized controlled ESCAPE trial, intensified blood pressure control is recommended in children with chronic kidney disease prior to kidney replacement therapy. However, current treatment recommendations for pediatric kidney transplant patients follow the recommendations for otherwise healthy children and adolescents with arterial hypertension, i.e., suggesting a blood pressure target < 90th percentile.</p><p><strong>Methods: </strong>In the proposed multicenter, randomized, parallel group trial with blinded endpoint evaluation, we aim to include 170 pediatric patients who underwent a kidney transplantation more than 12 months ago. Patients will be randomly assigned 1:1 to an intensified blood pressure management group (blood pressure target ≤ 60th percentile) and a standard blood pressure management group (blood pressure target < 90th percentile). The primary endpoint is left ventricular mass after 24 months. Secondary endpoints are pulse wave velocity, intima media thickness, estimated glomerular filtration rate, and albuminuria. Achievement of blood pressure targets will be facilitated through blood pressure telemonitoring. Blood pressure values will be transmitted in real time to the treating physician and the trial's centralized study office allowing timely responses in case blood pressure values lie outside target range.</p><p><strong>Discussion: </strong>The proposed study will result in an evidence-based definition of blood pressure targets and will therefore have direct implications for the care of children after kidney transplantation. In case intensified blood pressure targets are effective, this should eventually lead to lower cardiovascular morbidity and subsequently lower cardiovascular mortality of pediatric kidney transplant recipients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT06589947. Registered on September 6, 2024.</p>","PeriodicalId":23333,"journal":{"name":"Trials","volume":"26 1","pages":"315"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392664/pdf/","citationCount":"0","resultStr":"{\"title\":\"StOPping Hypertension and imprOving Children's Lives after KidnEy TranSplantation (SOPHOCLES): study protocol for a randomized controlled multicenter trial.\",\"authors\":\"Carl Grabitz, Nima Memaran, Rizky I Sugianto, Jeanine von der Born, Mila Bukova, Elena Lehmann, Ann-Kathrin Konuhov, Dennis Holzwart, Anika Großhennig, Elke Wühl, Bernhard M W Schmidt, Anette Melk\",\"doi\":\"10.1186/s13063-025-09033-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiovascular disease is a major morbidity in children after kidney transplantation, limiting life expectancy and impairing graft function. Arterial hypertension is the dominant cardiovascular risk factor and highly abundant in this patient group. Arterial hypertension can cause left ventricular hypertrophy, which is predictive of cardiovascular death. Left ventricular hypertrophy can be non-invasively assessed by measuring left ventricular mass. Observational data indicated that intensified blood pressure control was associated with a significant reduction of left ventricular mass. Based on evidence from the randomized controlled ESCAPE trial, intensified blood pressure control is recommended in children with chronic kidney disease prior to kidney replacement therapy. However, current treatment recommendations for pediatric kidney transplant patients follow the recommendations for otherwise healthy children and adolescents with arterial hypertension, i.e., suggesting a blood pressure target < 90th percentile.</p><p><strong>Methods: </strong>In the proposed multicenter, randomized, parallel group trial with blinded endpoint evaluation, we aim to include 170 pediatric patients who underwent a kidney transplantation more than 12 months ago. Patients will be randomly assigned 1:1 to an intensified blood pressure management group (blood pressure target ≤ 60th percentile) and a standard blood pressure management group (blood pressure target < 90th percentile). The primary endpoint is left ventricular mass after 24 months. Secondary endpoints are pulse wave velocity, intima media thickness, estimated glomerular filtration rate, and albuminuria. Achievement of blood pressure targets will be facilitated through blood pressure telemonitoring. Blood pressure values will be transmitted in real time to the treating physician and the trial's centralized study office allowing timely responses in case blood pressure values lie outside target range.</p><p><strong>Discussion: </strong>The proposed study will result in an evidence-based definition of blood pressure targets and will therefore have direct implications for the care of children after kidney transplantation. In case intensified blood pressure targets are effective, this should eventually lead to lower cardiovascular morbidity and subsequently lower cardiovascular mortality of pediatric kidney transplant recipients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT06589947. Registered on September 6, 2024.</p>\",\"PeriodicalId\":23333,\"journal\":{\"name\":\"Trials\",\"volume\":\"26 1\",\"pages\":\"315\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392664/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Trials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13063-025-09033-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13063-025-09033-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
StOPping Hypertension and imprOving Children's Lives after KidnEy TranSplantation (SOPHOCLES): study protocol for a randomized controlled multicenter trial.
Background: Cardiovascular disease is a major morbidity in children after kidney transplantation, limiting life expectancy and impairing graft function. Arterial hypertension is the dominant cardiovascular risk factor and highly abundant in this patient group. Arterial hypertension can cause left ventricular hypertrophy, which is predictive of cardiovascular death. Left ventricular hypertrophy can be non-invasively assessed by measuring left ventricular mass. Observational data indicated that intensified blood pressure control was associated with a significant reduction of left ventricular mass. Based on evidence from the randomized controlled ESCAPE trial, intensified blood pressure control is recommended in children with chronic kidney disease prior to kidney replacement therapy. However, current treatment recommendations for pediatric kidney transplant patients follow the recommendations for otherwise healthy children and adolescents with arterial hypertension, i.e., suggesting a blood pressure target < 90th percentile.
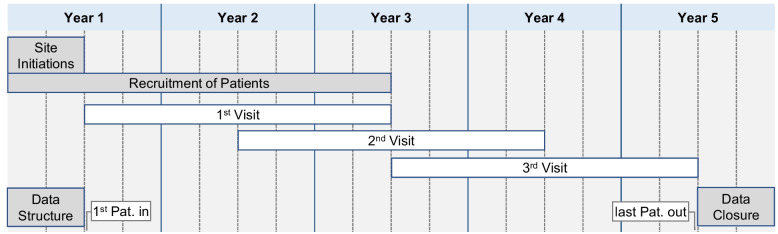
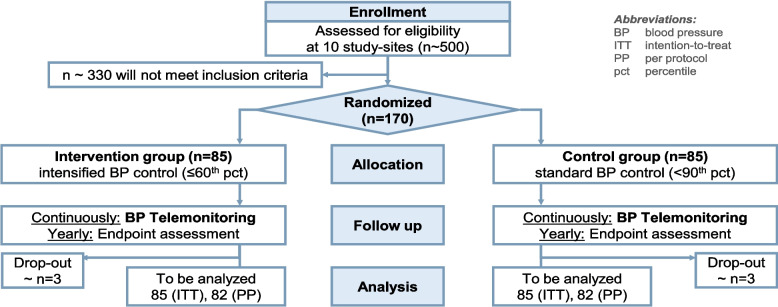
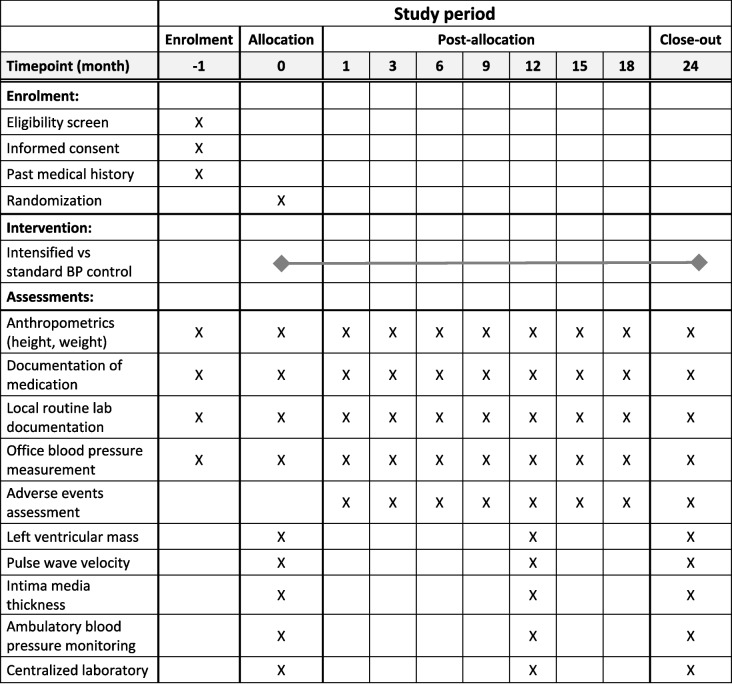
Methods: In the proposed multicenter, randomized, parallel group trial with blinded endpoint evaluation, we aim to include 170 pediatric patients who underwent a kidney transplantation more than 12 months ago. Patients will be randomly assigned 1:1 to an intensified blood pressure management group (blood pressure target ≤ 60th percentile) and a standard blood pressure management group (blood pressure target < 90th percentile). The primary endpoint is left ventricular mass after 24 months. Secondary endpoints are pulse wave velocity, intima media thickness, estimated glomerular filtration rate, and albuminuria. Achievement of blood pressure targets will be facilitated through blood pressure telemonitoring. Blood pressure values will be transmitted in real time to the treating physician and the trial's centralized study office allowing timely responses in case blood pressure values lie outside target range.
Discussion: The proposed study will result in an evidence-based definition of blood pressure targets and will therefore have direct implications for the care of children after kidney transplantation. In case intensified blood pressure targets are effective, this should eventually lead to lower cardiovascular morbidity and subsequently lower cardiovascular mortality of pediatric kidney transplant recipients.
Trial registration: ClinicalTrials.gov NCT06589947. Registered on September 6, 2024.
期刊介绍:
Trials is an open access, peer-reviewed, online journal that will encompass all aspects of the performance and findings of randomized controlled trials. Trials will experiment with, and then refine, innovative approaches to improving communication about trials. We are keen to move beyond publishing traditional trial results articles (although these will be included). We believe this represents an exciting opportunity to advance the science and reporting of trials. Prior to 2006, Trials was published as Current Controlled Trials in Cardiovascular Medicine (CCTCVM). All published CCTCVM articles are available via the Trials website and citations to CCTCVM article URLs will continue to be supported.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


