Christian Rønn, Barbara Bonnesen, Imane Achir Alispahic, Louise Lindhardt Tønnesen, Jakob Lyngby Kjærgaard, Mia Moberg, Charlotte Suppli Ulrik, Zitta Barrella Harboe, Andrea Browatzki, Torben Tranborg Jensen, Christian N Meyer, Uffe Bodtger, Elisabeth Bendstrup, Sofie Lock Johansson, Diana Utech Kaiser, Charlotte Hyldgaard, Jørgen Vestbo, Pradeesh Sivapalan, Jens-Ulrik Stæhr Jensen
{"title":"研究方案:COPD-嗜酸性粒细胞引导下减少吸入皮质类固醇(COPERNICOS):一项随机、双盲、多中心、四组干预临床试验,研究重度或极重度慢性阻塞性肺疾病(COPD)患者嗜酸性粒细胞引导下时间更新的个人特异性减少吸入皮质类固醇治疗和预防性低剂量阿奇霉素治疗。","authors":"Christian Rønn, Barbara Bonnesen, Imane Achir Alispahic, Louise Lindhardt Tønnesen, Jakob Lyngby Kjærgaard, Mia Moberg, Charlotte Suppli Ulrik, Zitta Barrella Harboe, Andrea Browatzki, Torben Tranborg Jensen, Christian N Meyer, Uffe Bodtger, Elisabeth Bendstrup, Sofie Lock Johansson, Diana Utech Kaiser, Charlotte Hyldgaard, Jørgen Vestbo, Pradeesh Sivapalan, Jens-Ulrik Stæhr Jensen","doi":"10.1186/s13063-025-09032-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inhaled corticosteroid (ICS) is frequently used for COPD. Based on the considerable adverse effects and the knowledge that many such patients do not gain benefit from this treatment, it remains unresolved whether ICS treatment can be managed with lower doses, or via an ICS-sparing strategy with periods with and without this medicine. The blood eosinophil count is a useful biomarker for steroid-responsive airway inflammation, and we want to investigate whether an individualized and eosinophil-guided approach on ICS treatment reduces ICS over-treatment and side effects. High-dose (500 mg thrice weekly or 250 mg daily) long-term azithromycin has been shown to reduce acute exacerbations of COPD in selected patients. Frequent gastro-intestinal adverse effects remain a challenge, but many patients tolerate lower doses; however, the effect of the treatment at lower doses is unknown, although many physicians prefer such doses. We want to investigate whether oral low-dose prophylactic azithromycin 250 mg three times weekly reduces acute exacerbations of COPD and improves time alive and out of hospital.</p><p><strong>Methods: </strong>This is an ongoing, actively recruiting randomized, double-blinded, multicenter, four-arm factorial intervention clinical trial aiming to recruit 444 patients with specialist verified COPD GOLD risk class E and/or FEV1 < 30% who are currently on ICS. The patients are followed for one year and are randomized 1:1:1:1 to one of the four treatment arms: (1) eosinophil-guided ICS-sparing treatment and low-dose azithromycin, (2) eosinophil-guided ICS treatment and placebo, (3) continued ICS treatment and low-dose azithromycin, or (4) continued ICS treatment and placebo. If blood-eosinophils (measured every 3 months) are < 0.3 × 10<sup>9</sup> cells/L, ICS treatment will be paused in the arms with eosinophil-guided ICS-sparing treatment. Azithromycin/placebo is double-blinded and administered three times weekly. The primary endpoint is the number of hospitalization-requiring COPD exacerbations and/or death within 365 days.</p><p><strong>Discussion: </strong>Severe ICS-adverse effects like bacterial infections should be reduced. The ICS-sparing intervention, we test, may provide a useful tool to do this safely. Azithromycin low-dose prophylaxis is practiced by many physicians. This trial will provide evidence of whether this is effective.</p><p><strong>Trial registration: </strong>ClinTrials.gov. NCT04481555. Registered on 14 AUG 2020, https://clinicaltrials.gov/study/NCT04481555 .</p>","PeriodicalId":23333,"journal":{"name":"Trials","volume":"26 1","pages":"335"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12403334/pdf/","citationCount":"0","resultStr":"{\"title\":\"Study protocol: COPD-eosinophil-guided reduction of inhaled corticosteroids (COPERNICOS) : A randomized, double-blinded, multicenter, four-arm intervention clinical trial on eosinophil-guided time-updated person-specific reduction of inhaled corticosteroid therapy and prophylactic low dose Azithromycin therapy in patients with severe or very severe chronic obstructive pulmonary disease (COPD).\",\"authors\":\"Christian Rønn, Barbara Bonnesen, Imane Achir Alispahic, Louise Lindhardt Tønnesen, Jakob Lyngby Kjærgaard, Mia Moberg, Charlotte Suppli Ulrik, Zitta Barrella Harboe, Andrea Browatzki, Torben Tranborg Jensen, Christian N Meyer, Uffe Bodtger, Elisabeth Bendstrup, Sofie Lock Johansson, Diana Utech Kaiser, Charlotte Hyldgaard, Jørgen Vestbo, Pradeesh Sivapalan, Jens-Ulrik Stæhr Jensen\",\"doi\":\"10.1186/s13063-025-09032-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Inhaled corticosteroid (ICS) is frequently used for COPD. Based on the considerable adverse effects and the knowledge that many such patients do not gain benefit from this treatment, it remains unresolved whether ICS treatment can be managed with lower doses, or via an ICS-sparing strategy with periods with and without this medicine. The blood eosinophil count is a useful biomarker for steroid-responsive airway inflammation, and we want to investigate whether an individualized and eosinophil-guided approach on ICS treatment reduces ICS over-treatment and side effects. High-dose (500 mg thrice weekly or 250 mg daily) long-term azithromycin has been shown to reduce acute exacerbations of COPD in selected patients. Frequent gastro-intestinal adverse effects remain a challenge, but many patients tolerate lower doses; however, the effect of the treatment at lower doses is unknown, although many physicians prefer such doses. We want to investigate whether oral low-dose prophylactic azithromycin 250 mg three times weekly reduces acute exacerbations of COPD and improves time alive and out of hospital.</p><p><strong>Methods: </strong>This is an ongoing, actively recruiting randomized, double-blinded, multicenter, four-arm factorial intervention clinical trial aiming to recruit 444 patients with specialist verified COPD GOLD risk class E and/or FEV1 < 30% who are currently on ICS. The patients are followed for one year and are randomized 1:1:1:1 to one of the four treatment arms: (1) eosinophil-guided ICS-sparing treatment and low-dose azithromycin, (2) eosinophil-guided ICS treatment and placebo, (3) continued ICS treatment and low-dose azithromycin, or (4) continued ICS treatment and placebo. If blood-eosinophils (measured every 3 months) are < 0.3 × 10<sup>9</sup> cells/L, ICS treatment will be paused in the arms with eosinophil-guided ICS-sparing treatment. Azithromycin/placebo is double-blinded and administered three times weekly. The primary endpoint is the number of hospitalization-requiring COPD exacerbations and/or death within 365 days.</p><p><strong>Discussion: </strong>Severe ICS-adverse effects like bacterial infections should be reduced. The ICS-sparing intervention, we test, may provide a useful tool to do this safely. Azithromycin low-dose prophylaxis is practiced by many physicians. This trial will provide evidence of whether this is effective.</p><p><strong>Trial registration: </strong>ClinTrials.gov. NCT04481555. Registered on 14 AUG 2020, https://clinicaltrials.gov/study/NCT04481555 .</p>\",\"PeriodicalId\":23333,\"journal\":{\"name\":\"Trials\",\"volume\":\"26 1\",\"pages\":\"335\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12403334/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Trials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13063-025-09032-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13063-025-09032-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Study protocol: COPD-eosinophil-guided reduction of inhaled corticosteroids (COPERNICOS) : A randomized, double-blinded, multicenter, four-arm intervention clinical trial on eosinophil-guided time-updated person-specific reduction of inhaled corticosteroid therapy and prophylactic low dose Azithromycin therapy in patients with severe or very severe chronic obstructive pulmonary disease (COPD).
Background: Inhaled corticosteroid (ICS) is frequently used for COPD. Based on the considerable adverse effects and the knowledge that many such patients do not gain benefit from this treatment, it remains unresolved whether ICS treatment can be managed with lower doses, or via an ICS-sparing strategy with periods with and without this medicine. The blood eosinophil count is a useful biomarker for steroid-responsive airway inflammation, and we want to investigate whether an individualized and eosinophil-guided approach on ICS treatment reduces ICS over-treatment and side effects. High-dose (500 mg thrice weekly or 250 mg daily) long-term azithromycin has been shown to reduce acute exacerbations of COPD in selected patients. Frequent gastro-intestinal adverse effects remain a challenge, but many patients tolerate lower doses; however, the effect of the treatment at lower doses is unknown, although many physicians prefer such doses. We want to investigate whether oral low-dose prophylactic azithromycin 250 mg three times weekly reduces acute exacerbations of COPD and improves time alive and out of hospital.
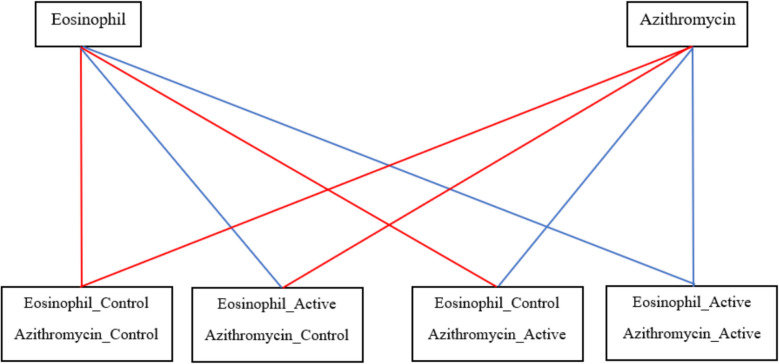
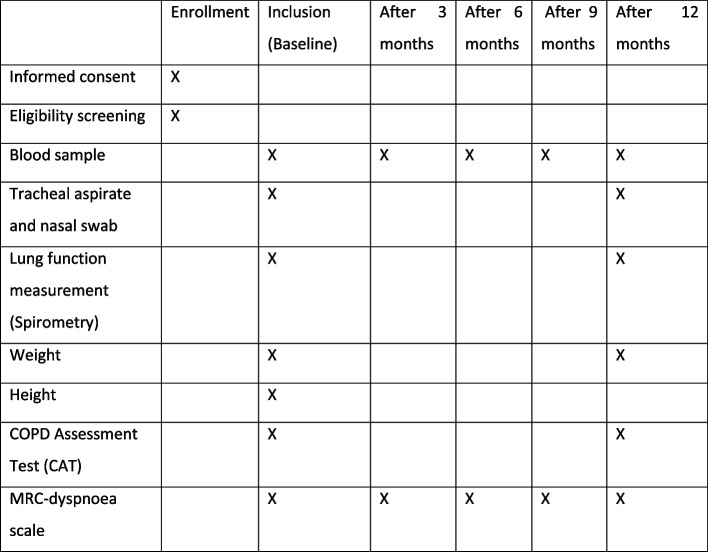
Methods: This is an ongoing, actively recruiting randomized, double-blinded, multicenter, four-arm factorial intervention clinical trial aiming to recruit 444 patients with specialist verified COPD GOLD risk class E and/or FEV1 < 30% who are currently on ICS. The patients are followed for one year and are randomized 1:1:1:1 to one of the four treatment arms: (1) eosinophil-guided ICS-sparing treatment and low-dose azithromycin, (2) eosinophil-guided ICS treatment and placebo, (3) continued ICS treatment and low-dose azithromycin, or (4) continued ICS treatment and placebo. If blood-eosinophils (measured every 3 months) are < 0.3 × 109 cells/L, ICS treatment will be paused in the arms with eosinophil-guided ICS-sparing treatment. Azithromycin/placebo is double-blinded and administered three times weekly. The primary endpoint is the number of hospitalization-requiring COPD exacerbations and/or death within 365 days.
Discussion: Severe ICS-adverse effects like bacterial infections should be reduced. The ICS-sparing intervention, we test, may provide a useful tool to do this safely. Azithromycin low-dose prophylaxis is practiced by many physicians. This trial will provide evidence of whether this is effective.
Trial registration: ClinTrials.gov. NCT04481555. Registered on 14 AUG 2020, https://clinicaltrials.gov/study/NCT04481555 .
期刊介绍:
Trials is an open access, peer-reviewed, online journal that will encompass all aspects of the performance and findings of randomized controlled trials. Trials will experiment with, and then refine, innovative approaches to improving communication about trials. We are keen to move beyond publishing traditional trial results articles (although these will be included). We believe this represents an exciting opportunity to advance the science and reporting of trials. Prior to 2006, Trials was published as Current Controlled Trials in Cardiovascular Medicine (CCTCVM). All published CCTCVM articles are available via the Trials website and citations to CCTCVM article URLs will continue to be supported.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


