{"title":"优化急性胆管炎患者的短期抗生素治疗:一项开放标签随机对照试验(BOLT-P3试验)的研究方案","authors":"Sakue Masuda, Yoshinori Imamura, Karen Kimura, Makomo Makazu, Jun Kubota, Hiroshi Takihara, Ryuhei Jinushi, Tomoaki Fujikawa, Kyohei Maejima, Aya Kawanishi, Ryuichi Yamamoto, Shogo Noda, Taiji Koyama, Ayumu Sugitani, Shomei Ryozawa, Kazuya Koizumi","doi":"10.1186/s13063-025-09077-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute cholangitis (AC) frequently presents as a community-acquired infection and is associated with a high prevalence of antibiotic use among infectious diseases. The Tokyo Guidelines 2018 (TG18) recommend 4-7 days of antibiotic administration after biliary drainage. However, this recommendation lacks strong evidence of its effectiveness and is primarily based on heterogeneous clinical findings and expert opinions. Recent retrospective studies have advocated a shorter 1- to 3-day antibiotic course as effective for AC treatment, prompting the need to reassess the treatment duration to achieve therapeutic efficacy while minimizing resistance and adverse effects.</p><p><strong>Methods: </strong>We designed a multicenter, non-blinded, randomized trial to evaluate the efficacy of short-course therapy compared to standard-course therapy for AC management. The short-course therapy group will receive 1-3 days of intravenous (IV) antibiotic treatment after successful biliary drainage compared to 4-7 days of IV antibiotics after successful biliary drainage for the standard-course therapy group. The primary outcome is the clinical cure rate within 14 days from the endoscopic retrograde cholangiopancreatography (ERCP) procedure. Participants will be allocated to either treatment course using a minimization method in a non-blinded, randomized manner, with stratification factors including condition severity and facility. We determined that 210 participants would be required to achieve a statistical power of 90% with a one-sided significance threshold of 2.5% and a non-inferiority limit of 10%.</p><p><strong>Discussion: </strong>This phase 3 trial aims to determine the non-inferiority of short-course therapy over standard-course therapy. Shortening the duration of antibiotic administration may mitigate the emergence of resistant bacteria, adverse events, and reduce hospital stay length and healthcare costs. https://jrct.niph.go.jp/re/reports/detail/73862 TRIAL REGISTRATION: This study was registered at the Japan Registry of Clinical Trials under registry number jRCT1031230709. Registered on 14 March 2024, https://jrct.niph.go.jp/re/reports/detail/73862.</p>","PeriodicalId":23333,"journal":{"name":"Trials","volume":"26 1","pages":"324"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400583/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimizing short-term antibiotic treatment in patients with acute cholangitis: study protocol for an open-label randomized controlled trial (the BOLT-P3 trial).\",\"authors\":\"Sakue Masuda, Yoshinori Imamura, Karen Kimura, Makomo Makazu, Jun Kubota, Hiroshi Takihara, Ryuhei Jinushi, Tomoaki Fujikawa, Kyohei Maejima, Aya Kawanishi, Ryuichi Yamamoto, Shogo Noda, Taiji Koyama, Ayumu Sugitani, Shomei Ryozawa, Kazuya Koizumi\",\"doi\":\"10.1186/s13063-025-09077-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute cholangitis (AC) frequently presents as a community-acquired infection and is associated with a high prevalence of antibiotic use among infectious diseases. The Tokyo Guidelines 2018 (TG18) recommend 4-7 days of antibiotic administration after biliary drainage. However, this recommendation lacks strong evidence of its effectiveness and is primarily based on heterogeneous clinical findings and expert opinions. Recent retrospective studies have advocated a shorter 1- to 3-day antibiotic course as effective for AC treatment, prompting the need to reassess the treatment duration to achieve therapeutic efficacy while minimizing resistance and adverse effects.</p><p><strong>Methods: </strong>We designed a multicenter, non-blinded, randomized trial to evaluate the efficacy of short-course therapy compared to standard-course therapy for AC management. The short-course therapy group will receive 1-3 days of intravenous (IV) antibiotic treatment after successful biliary drainage compared to 4-7 days of IV antibiotics after successful biliary drainage for the standard-course therapy group. The primary outcome is the clinical cure rate within 14 days from the endoscopic retrograde cholangiopancreatography (ERCP) procedure. Participants will be allocated to either treatment course using a minimization method in a non-blinded, randomized manner, with stratification factors including condition severity and facility. We determined that 210 participants would be required to achieve a statistical power of 90% with a one-sided significance threshold of 2.5% and a non-inferiority limit of 10%.</p><p><strong>Discussion: </strong>This phase 3 trial aims to determine the non-inferiority of short-course therapy over standard-course therapy. Shortening the duration of antibiotic administration may mitigate the emergence of resistant bacteria, adverse events, and reduce hospital stay length and healthcare costs. https://jrct.niph.go.jp/re/reports/detail/73862 TRIAL REGISTRATION: This study was registered at the Japan Registry of Clinical Trials under registry number jRCT1031230709. Registered on 14 March 2024, https://jrct.niph.go.jp/re/reports/detail/73862.</p>\",\"PeriodicalId\":23333,\"journal\":{\"name\":\"Trials\",\"volume\":\"26 1\",\"pages\":\"324\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400583/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Trials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13063-025-09077-1\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13063-025-09077-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Optimizing short-term antibiotic treatment in patients with acute cholangitis: study protocol for an open-label randomized controlled trial (the BOLT-P3 trial).
Background: Acute cholangitis (AC) frequently presents as a community-acquired infection and is associated with a high prevalence of antibiotic use among infectious diseases. The Tokyo Guidelines 2018 (TG18) recommend 4-7 days of antibiotic administration after biliary drainage. However, this recommendation lacks strong evidence of its effectiveness and is primarily based on heterogeneous clinical findings and expert opinions. Recent retrospective studies have advocated a shorter 1- to 3-day antibiotic course as effective for AC treatment, prompting the need to reassess the treatment duration to achieve therapeutic efficacy while minimizing resistance and adverse effects.
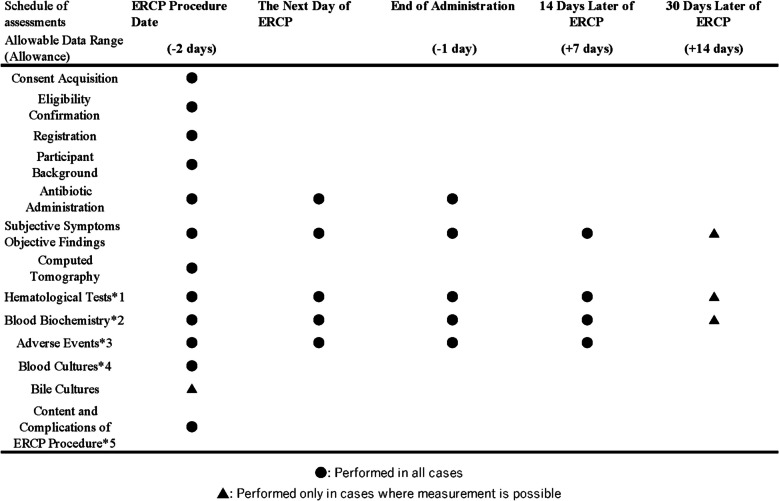
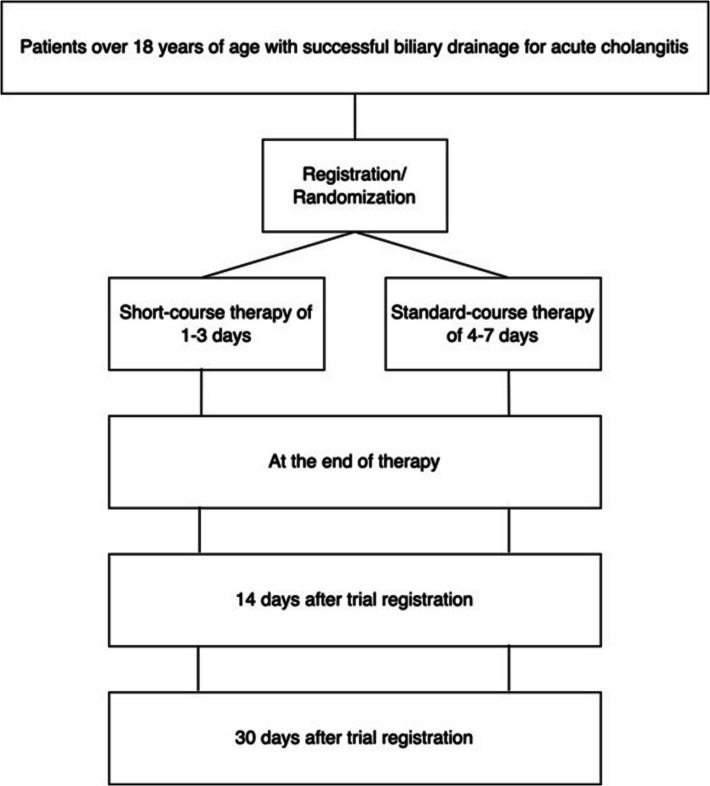
Methods: We designed a multicenter, non-blinded, randomized trial to evaluate the efficacy of short-course therapy compared to standard-course therapy for AC management. The short-course therapy group will receive 1-3 days of intravenous (IV) antibiotic treatment after successful biliary drainage compared to 4-7 days of IV antibiotics after successful biliary drainage for the standard-course therapy group. The primary outcome is the clinical cure rate within 14 days from the endoscopic retrograde cholangiopancreatography (ERCP) procedure. Participants will be allocated to either treatment course using a minimization method in a non-blinded, randomized manner, with stratification factors including condition severity and facility. We determined that 210 participants would be required to achieve a statistical power of 90% with a one-sided significance threshold of 2.5% and a non-inferiority limit of 10%.
Discussion: This phase 3 trial aims to determine the non-inferiority of short-course therapy over standard-course therapy. Shortening the duration of antibiotic administration may mitigate the emergence of resistant bacteria, adverse events, and reduce hospital stay length and healthcare costs. https://jrct.niph.go.jp/re/reports/detail/73862 TRIAL REGISTRATION: This study was registered at the Japan Registry of Clinical Trials under registry number jRCT1031230709. Registered on 14 March 2024, https://jrct.niph.go.jp/re/reports/detail/73862.
期刊介绍:
Trials is an open access, peer-reviewed, online journal that will encompass all aspects of the performance and findings of randomized controlled trials. Trials will experiment with, and then refine, innovative approaches to improving communication about trials. We are keen to move beyond publishing traditional trial results articles (although these will be included). We believe this represents an exciting opportunity to advance the science and reporting of trials. Prior to 2006, Trials was published as Current Controlled Trials in Cardiovascular Medicine (CCTCVM). All published CCTCVM articles are available via the Trials website and citations to CCTCVM article URLs will continue to be supported.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


