Kelvin Yan, Arizah Bakhtiah, Shweta Hota, Joanne Evans, Frankie Mo
{"title":"T790M突变检测和序贯奥西替尼治疗egfr阳性晚期非小细胞肺癌的实际结果:重新审视的策略","authors":"Kelvin Yan, Arizah Bakhtiah, Shweta Hota, Joanne Evans, Frankie Mo","doi":"10.1007/s11523-025-01173-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Epidermal growth factor receptor (EGFR)-driven non-small cell lung cancer (eLC) is a leading cause of death. The FLAURA study showed that upfront osimertinib (U-OSI) led to better overall survival (OS) than gefitinib or erlotinib, regardless of T790M status in advanced disease. However, if sequenced optimally, sequential OSI (S-OSI) in T790M-positive patients after first- or second-generation EGFR-tyrosine kinase inhibitors (F-S-EGFR-TKI) should theoretically lead to better OS than U-OSI.</p><p><strong>Objective: </strong>To identify the best sequencing strategy in this group of patients.</p><p><strong>Patients and methods: </strong>A multicentre retrospective study was conducted on treatment-naive eLC patients who had received an F-S- EGFR-TKI between 1 January 2016 and 31 December 2020 in three tertiary NHS hospitals in the UK. Compliance to national recommendation of T790M testing was analysed. Survival outcomes of T790M testing and S-OSI were estimated with the Kaplan-Meier and Cox Proportional Hazard models.</p><p><strong>Results: </strong>In 84/122 evaluable patients, after F-S-EGFR-TKI, only 50% of the patients were offered a T790M biopsy, owing to rapid progression and reduced fitness. Of which, 59.5% of the patients tested positive and had S-OSI. Median OS for the T790M-tested cohort, regardless of positivity and S-OSI, was 54.0 months vs 8.9 months in those not tested (P = < 0.001). Median OS of S-OSI in T790M-positive patients was 64.0 months vs 34.9 months in the T790M-negative cohort (P < 0.0001). On multivariable analysis, S-OSI was associated with better OS (HR 1.841; 95% CI 1.052-3.221; P = 0.0325), whereas performance status (HR 2. 256; 95% CI 1.151-4.422, P = 0.0178), presence of baseline intracranial disease (HR 2 .022; 95% CI 1.144-3.575, P = 0. 0115), the male sex (HR 2.265; 95% CI 1.302-3.939; P = 0.0038) and non-exon 19 deletion mutations (HR 1.610; 95% CI 1.112-2.331, P = 0.0116) were associated with a higher risk of death.</p><p><strong>Conclusions: </strong>High performance status and intracranial disease should be indications for U-OSI for a higher chance of response. For fitter patients, F-S-EGFR-TKI followed by T790M biopsy +/- S-OSI appears to confer better-than-expected OS in the entire cohort in the real-world setting, regardless of T790M positivity. Given the clinical benefit and potential cost-effectiveness of this approach, S-OSI should be considered a favourable option in this group of patients, especially in resource-deprived settings.</p>","PeriodicalId":22195,"journal":{"name":"Targeted Oncology","volume":" ","pages":"861-870"},"PeriodicalIF":4.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454508/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-World Outcomes of T790M Mutation Testing and Sequential Osimertinib in EGFR-Positive Advanced Non-small Cell Lung Cancer: A Revisited Strategy.\",\"authors\":\"Kelvin Yan, Arizah Bakhtiah, Shweta Hota, Joanne Evans, Frankie Mo\",\"doi\":\"10.1007/s11523-025-01173-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Epidermal growth factor receptor (EGFR)-driven non-small cell lung cancer (eLC) is a leading cause of death. The FLAURA study showed that upfront osimertinib (U-OSI) led to better overall survival (OS) than gefitinib or erlotinib, regardless of T790M status in advanced disease. However, if sequenced optimally, sequential OSI (S-OSI) in T790M-positive patients after first- or second-generation EGFR-tyrosine kinase inhibitors (F-S-EGFR-TKI) should theoretically lead to better OS than U-OSI.</p><p><strong>Objective: </strong>To identify the best sequencing strategy in this group of patients.</p><p><strong>Patients and methods: </strong>A multicentre retrospective study was conducted on treatment-naive eLC patients who had received an F-S- EGFR-TKI between 1 January 2016 and 31 December 2020 in three tertiary NHS hospitals in the UK. Compliance to national recommendation of T790M testing was analysed. Survival outcomes of T790M testing and S-OSI were estimated with the Kaplan-Meier and Cox Proportional Hazard models.</p><p><strong>Results: </strong>In 84/122 evaluable patients, after F-S-EGFR-TKI, only 50% of the patients were offered a T790M biopsy, owing to rapid progression and reduced fitness. Of which, 59.5% of the patients tested positive and had S-OSI. Median OS for the T790M-tested cohort, regardless of positivity and S-OSI, was 54.0 months vs 8.9 months in those not tested (P = < 0.001). Median OS of S-OSI in T790M-positive patients was 64.0 months vs 34.9 months in the T790M-negative cohort (P < 0.0001). On multivariable analysis, S-OSI was associated with better OS (HR 1.841; 95% CI 1.052-3.221; P = 0.0325), whereas performance status (HR 2. 256; 95% CI 1.151-4.422, P = 0.0178), presence of baseline intracranial disease (HR 2 .022; 95% CI 1.144-3.575, P = 0. 0115), the male sex (HR 2.265; 95% CI 1.302-3.939; P = 0.0038) and non-exon 19 deletion mutations (HR 1.610; 95% CI 1.112-2.331, P = 0.0116) were associated with a higher risk of death.</p><p><strong>Conclusions: </strong>High performance status and intracranial disease should be indications for U-OSI for a higher chance of response. For fitter patients, F-S-EGFR-TKI followed by T790M biopsy +/- S-OSI appears to confer better-than-expected OS in the entire cohort in the real-world setting, regardless of T790M positivity. Given the clinical benefit and potential cost-effectiveness of this approach, S-OSI should be considered a favourable option in this group of patients, especially in resource-deprived settings.</p>\",\"PeriodicalId\":22195,\"journal\":{\"name\":\"Targeted Oncology\",\"volume\":\" \",\"pages\":\"861-870\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454508/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Targeted Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11523-025-01173-1\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Targeted Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11523-025-01173-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/2 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:表皮生长因子受体(EGFR)驱动的非小细胞肺癌(eLC)是导致死亡的主要原因。FLAURA研究表明,无论T790M是否处于晚期疾病,奥西替尼(U-OSI)的前期治疗比吉非替尼或厄洛替尼的总生存期(OS)更好。然而,如果测序最优,使用第一代或第二代egfr -酪氨酸激酶抑制剂(F-S-EGFR-TKI)的t790m阳性患者的顺序OSI (S-OSI)理论上应该比U-OSI带来更好的OS。目的:确定该患者的最佳测序策略。患者和方法:对2016年1月1日至2020年12月31日期间在英国三家三级NHS医院接受F-S- EGFR-TKI治疗的初治eLC患者进行了一项多中心回顾性研究。对国家推荐的T790M检测符合性进行分析。采用Kaplan-Meier和Cox比例风险模型估计T790M检测和S-OSI的生存结局。结果:在84/122例可评估的患者中,在F-S-EGFR-TKI后,由于进展迅速和适应性降低,只有50%的患者进行了T790M活检。其中,59.5%的患者检测呈阳性,患有S-OSI。t790m检测队列的中位生存期(不论阳性和S-OSI)为54.0个月,而未检测组为8.9个月(P = < 0.001)。t790m阳性患者S-OSI的中位生存期为64.0个月,而t790m阴性患者为34.9个月(P < 0.0001)。在多变量分析中,S-OSI与更好的OS相关(HR 1.841; 95% CI 1.052-3.221; P = 0.0325),而性能状态(HR 2。256年;95% CI 1.151-4.422, P = 0.0178),存在基线颅内疾病(HR 2.022; 95% CI 1.144-3.575, P = 0。0115)、男性(HR 2.265; 95% CI 1.302-3.939; P = 0.0038)和非外显子19缺失突变(HR 1.610; 95% CI 1.112-2.331, P = 0.0116)与较高的死亡风险相关。结论:高性能状态和颅内疾病应作为U-OSI的适应症,以获得更高的应答机会。对于健康状况较好的患者,F-S-EGFR-TKI随后进行T790M活检+/- S-OSI,无论T790M是否阳性,在现实环境中,整个队列的OS似乎都好于预期。考虑到这种方法的临床效益和潜在的成本效益,S-OSI应该被认为是这组患者的有利选择,特别是在资源匮乏的环境中。
Real-World Outcomes of T790M Mutation Testing and Sequential Osimertinib in EGFR-Positive Advanced Non-small Cell Lung Cancer: A Revisited Strategy.
Background: Epidermal growth factor receptor (EGFR)-driven non-small cell lung cancer (eLC) is a leading cause of death. The FLAURA study showed that upfront osimertinib (U-OSI) led to better overall survival (OS) than gefitinib or erlotinib, regardless of T790M status in advanced disease. However, if sequenced optimally, sequential OSI (S-OSI) in T790M-positive patients after first- or second-generation EGFR-tyrosine kinase inhibitors (F-S-EGFR-TKI) should theoretically lead to better OS than U-OSI.
Objective: To identify the best sequencing strategy in this group of patients.
Patients and methods: A multicentre retrospective study was conducted on treatment-naive eLC patients who had received an F-S- EGFR-TKI between 1 January 2016 and 31 December 2020 in three tertiary NHS hospitals in the UK. Compliance to national recommendation of T790M testing was analysed. Survival outcomes of T790M testing and S-OSI were estimated with the Kaplan-Meier and Cox Proportional Hazard models.
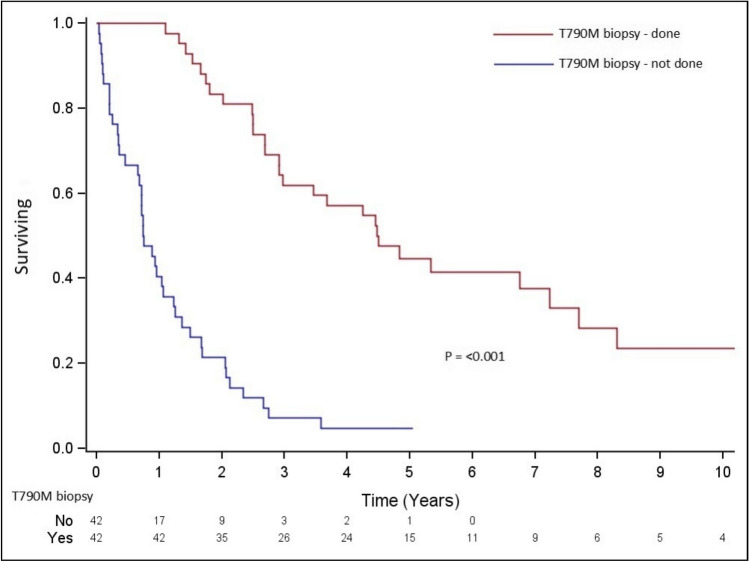
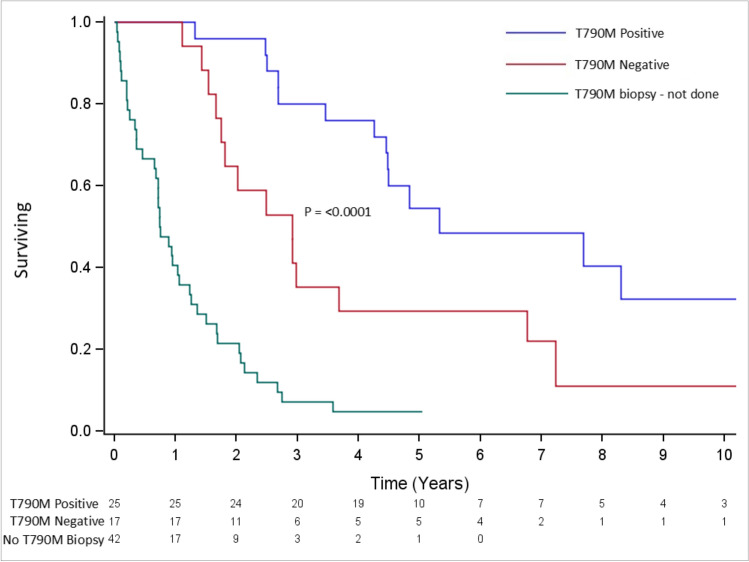
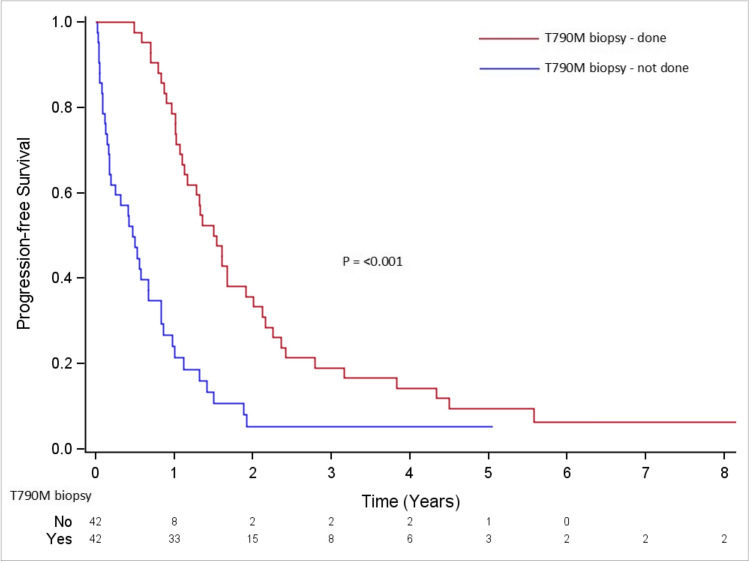
Results: In 84/122 evaluable patients, after F-S-EGFR-TKI, only 50% of the patients were offered a T790M biopsy, owing to rapid progression and reduced fitness. Of which, 59.5% of the patients tested positive and had S-OSI. Median OS for the T790M-tested cohort, regardless of positivity and S-OSI, was 54.0 months vs 8.9 months in those not tested (P = < 0.001). Median OS of S-OSI in T790M-positive patients was 64.0 months vs 34.9 months in the T790M-negative cohort (P < 0.0001). On multivariable analysis, S-OSI was associated with better OS (HR 1.841; 95% CI 1.052-3.221; P = 0.0325), whereas performance status (HR 2. 256; 95% CI 1.151-4.422, P = 0.0178), presence of baseline intracranial disease (HR 2 .022; 95% CI 1.144-3.575, P = 0. 0115), the male sex (HR 2.265; 95% CI 1.302-3.939; P = 0.0038) and non-exon 19 deletion mutations (HR 1.610; 95% CI 1.112-2.331, P = 0.0116) were associated with a higher risk of death.
Conclusions: High performance status and intracranial disease should be indications for U-OSI for a higher chance of response. For fitter patients, F-S-EGFR-TKI followed by T790M biopsy +/- S-OSI appears to confer better-than-expected OS in the entire cohort in the real-world setting, regardless of T790M positivity. Given the clinical benefit and potential cost-effectiveness of this approach, S-OSI should be considered a favourable option in this group of patients, especially in resource-deprived settings.
期刊介绍:
Targeted Oncology addresses physicians and scientists committed to oncology and cancer research by providing a programme of articles on molecularly targeted pharmacotherapy in oncology. The journal includes:
Original Research Articles on all aspects of molecularly targeted agents for the treatment of cancer, including immune checkpoint inhibitors and related approaches.
Comprehensive narrative Review Articles and shorter Leading Articles discussing relevant clinically established as well as emerging agents and pathways.
Current Opinion articles that place interesting areas in perspective.
Therapy in Practice articles that provide a guide to the optimum management of a condition and highlight practical, clinically relevant considerations and recommendations.
Systematic Reviews that use explicit, systematic methods as outlined by the PRISMA statement.
Adis Drug Reviews of the properties and place in therapy of both newer and established targeted drugs in oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


