Ailís Ceara Haney, Janek Salatzki, Andreas Ochs, Thomas Hilbel, Lukas D Weberling, Hauke Hund, Evangelos Giannitsis, Norbert Frey, Henning Steen, Dirk Lossnitzer, Florian André
{"title":"应激性心血管磁共振对缺血性心脏病左室射血分数严重降低患者的预后价值。","authors":"Ailís Ceara Haney, Janek Salatzki, Andreas Ochs, Thomas Hilbel, Lukas D Weberling, Hauke Hund, Evangelos Giannitsis, Norbert Frey, Henning Steen, Dirk Lossnitzer, Florian André","doi":"10.1136/openhrt-2025-003466","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The concept of ischaemia for therapeutic guidance and risk stratification in coronary artery disease has been challenged in recent years. In particular, there is limited understanding of the prognostic value of ischaemia in patients with severely reduced left ventricular ejection fraction (LVEF). The aim of this study was to investigate the prognostic value of stress cardiovascular magnetic resonance (stress CMR) in patients with ischaemic heart disease (IHD) and severely reduced LVEF.</p><p><strong>Methods: </strong>This retrospective study included patients with IHD and an LVEF ≤35% who underwent stress CMR between 2009 and 2022. The primary endpoint was the occurrence of a major adverse cardiovascular event (MACE), including cardiac death, non-fatal myocardial infarction (MI), survived sudden cardiac death and implanted cardioverter defibrillator shock for ventricular fibrillation. The secondary combined endpoint included heart failure hospitalisation, percutaneous coronary intervention, arrhythmia and coronary artery bypass grafting (CABG). All-cause death was also documented.</p><p><strong>Results: </strong>The study population consisted of 362 patients (85.6% men, 70.5 (63.0-78.0) years) with an LVEF of 30.2% (25.2%-33.0%). 245 patients (67.6%) had three vessel disease, 206 patients (57.2%) had a history of MI and 83 patients (22.9%) had a history of CABG. Stress CMR showed ischaemia in 72 (19.9%) patients. Among those, 32 patients (8.8%) underwent early revascularisation. Follow-up was 4.5 (3.0-6.6) years. MACE occurred in 101 patients (27.9%), including 41 cases of cardiac death (11.3%) and 40 cases of MI (11.0%). Ischaemia was not significantly associated with MACE, the combined secondary endpoint, or all-cause death in survival analysis (HR for MACE 1.20, 95% CI 0.74 to 1.95, p=0.4).</p><p><strong>Conclusion: </strong>In a cohort of patients with IHD and severely reduced LVEF, outcome did not differ when stratifying by ischaemia on stress CMR. We found no evidence that ischaemia could identify patients with increased risk for MACE, the combined secondary endpoint or all-cause death.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382561/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic value of stress cardiovascular magnetic resonance in patients with ischaemic heart disease and severely reduced left ventricular ejection fraction.\",\"authors\":\"Ailís Ceara Haney, Janek Salatzki, Andreas Ochs, Thomas Hilbel, Lukas D Weberling, Hauke Hund, Evangelos Giannitsis, Norbert Frey, Henning Steen, Dirk Lossnitzer, Florian André\",\"doi\":\"10.1136/openhrt-2025-003466\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The concept of ischaemia for therapeutic guidance and risk stratification in coronary artery disease has been challenged in recent years. In particular, there is limited understanding of the prognostic value of ischaemia in patients with severely reduced left ventricular ejection fraction (LVEF). The aim of this study was to investigate the prognostic value of stress cardiovascular magnetic resonance (stress CMR) in patients with ischaemic heart disease (IHD) and severely reduced LVEF.</p><p><strong>Methods: </strong>This retrospective study included patients with IHD and an LVEF ≤35% who underwent stress CMR between 2009 and 2022. The primary endpoint was the occurrence of a major adverse cardiovascular event (MACE), including cardiac death, non-fatal myocardial infarction (MI), survived sudden cardiac death and implanted cardioverter defibrillator shock for ventricular fibrillation. The secondary combined endpoint included heart failure hospitalisation, percutaneous coronary intervention, arrhythmia and coronary artery bypass grafting (CABG). All-cause death was also documented.</p><p><strong>Results: </strong>The study population consisted of 362 patients (85.6% men, 70.5 (63.0-78.0) years) with an LVEF of 30.2% (25.2%-33.0%). 245 patients (67.6%) had three vessel disease, 206 patients (57.2%) had a history of MI and 83 patients (22.9%) had a history of CABG. Stress CMR showed ischaemia in 72 (19.9%) patients. Among those, 32 patients (8.8%) underwent early revascularisation. Follow-up was 4.5 (3.0-6.6) years. MACE occurred in 101 patients (27.9%), including 41 cases of cardiac death (11.3%) and 40 cases of MI (11.0%). Ischaemia was not significantly associated with MACE, the combined secondary endpoint, or all-cause death in survival analysis (HR for MACE 1.20, 95% CI 0.74 to 1.95, p=0.4).</p><p><strong>Conclusion: </strong>In a cohort of patients with IHD and severely reduced LVEF, outcome did not differ when stratifying by ischaemia on stress CMR. We found no evidence that ischaemia could identify patients with increased risk for MACE, the combined secondary endpoint or all-cause death.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382561/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2025-003466\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003466","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:近年来,冠状动脉疾病的治疗指导和危险分层的缺血性概念受到了挑战。特别是,对于严重降低左心室射血分数(LVEF)患者的缺血预后价值的了解有限。本研究的目的是探讨应激性心血管磁共振(stress CMR)对缺血性心脏病(IHD)和LVEF严重降低患者的预后价值。方法:本回顾性研究纳入2009年至2022年间接受应激性CMR治疗的IHD和LVEF≤35%的患者。主要终点是主要不良心血管事件(MACE)的发生,包括心源性死亡、非致死性心肌梗死(MI)、存活的心源性猝死和因心室颤动而植入的心律转复除颤器休克。次要联合终点包括心力衰竭住院、经皮冠状动脉介入治疗、心律失常和冠状动脉旁路移植术(CABG)。全因死亡也有记录。结果:研究人群包括362例患者(85.6%为男性,70.5(63.0-78.0)岁),LVEF为30.2%(25.2%-33.0%)。三支血管病变245例(67.6%),心肌梗死史206例(57.2%),冠脉搭桥史83例(22.9%)。应激性CMR显示缺血性72例(19.9%)。其中32例(8.8%)患者接受了早期血运重建。随访时间为4.5年(3.0 ~ 6.6年)。MACE发生101例(27.9%),其中心源性死亡41例(11.3%),心肌梗死40例(11.0%)。在生存分析中,缺血与MACE、联合次要终点或全因死亡无显著相关(MACE的HR为1.20,95% CI 0.74至1.95,p=0.4)。结论:在IHD和LVEF严重降低的患者队列中,在应激CMR上按缺血程度分层的结果没有差异。我们没有发现任何证据表明缺血可以识别MACE、联合次要终点或全因死亡风险增加的患者。
Prognostic value of stress cardiovascular magnetic resonance in patients with ischaemic heart disease and severely reduced left ventricular ejection fraction.
Background: The concept of ischaemia for therapeutic guidance and risk stratification in coronary artery disease has been challenged in recent years. In particular, there is limited understanding of the prognostic value of ischaemia in patients with severely reduced left ventricular ejection fraction (LVEF). The aim of this study was to investigate the prognostic value of stress cardiovascular magnetic resonance (stress CMR) in patients with ischaemic heart disease (IHD) and severely reduced LVEF.
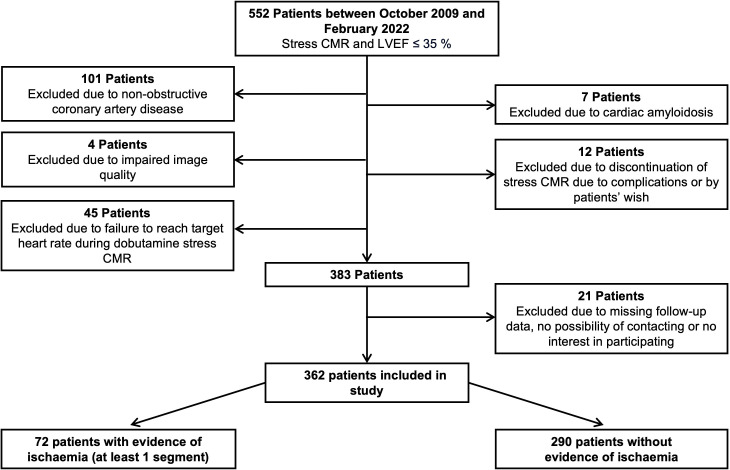
Methods: This retrospective study included patients with IHD and an LVEF ≤35% who underwent stress CMR between 2009 and 2022. The primary endpoint was the occurrence of a major adverse cardiovascular event (MACE), including cardiac death, non-fatal myocardial infarction (MI), survived sudden cardiac death and implanted cardioverter defibrillator shock for ventricular fibrillation. The secondary combined endpoint included heart failure hospitalisation, percutaneous coronary intervention, arrhythmia and coronary artery bypass grafting (CABG). All-cause death was also documented.
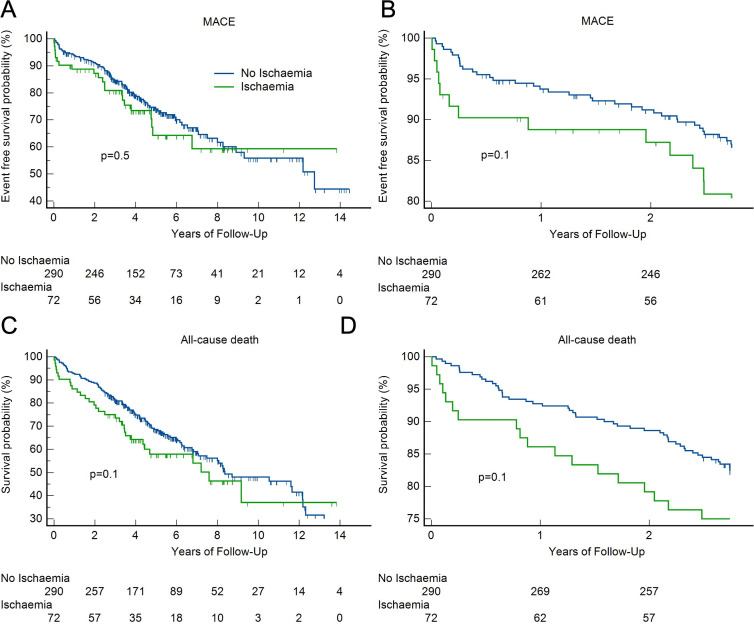
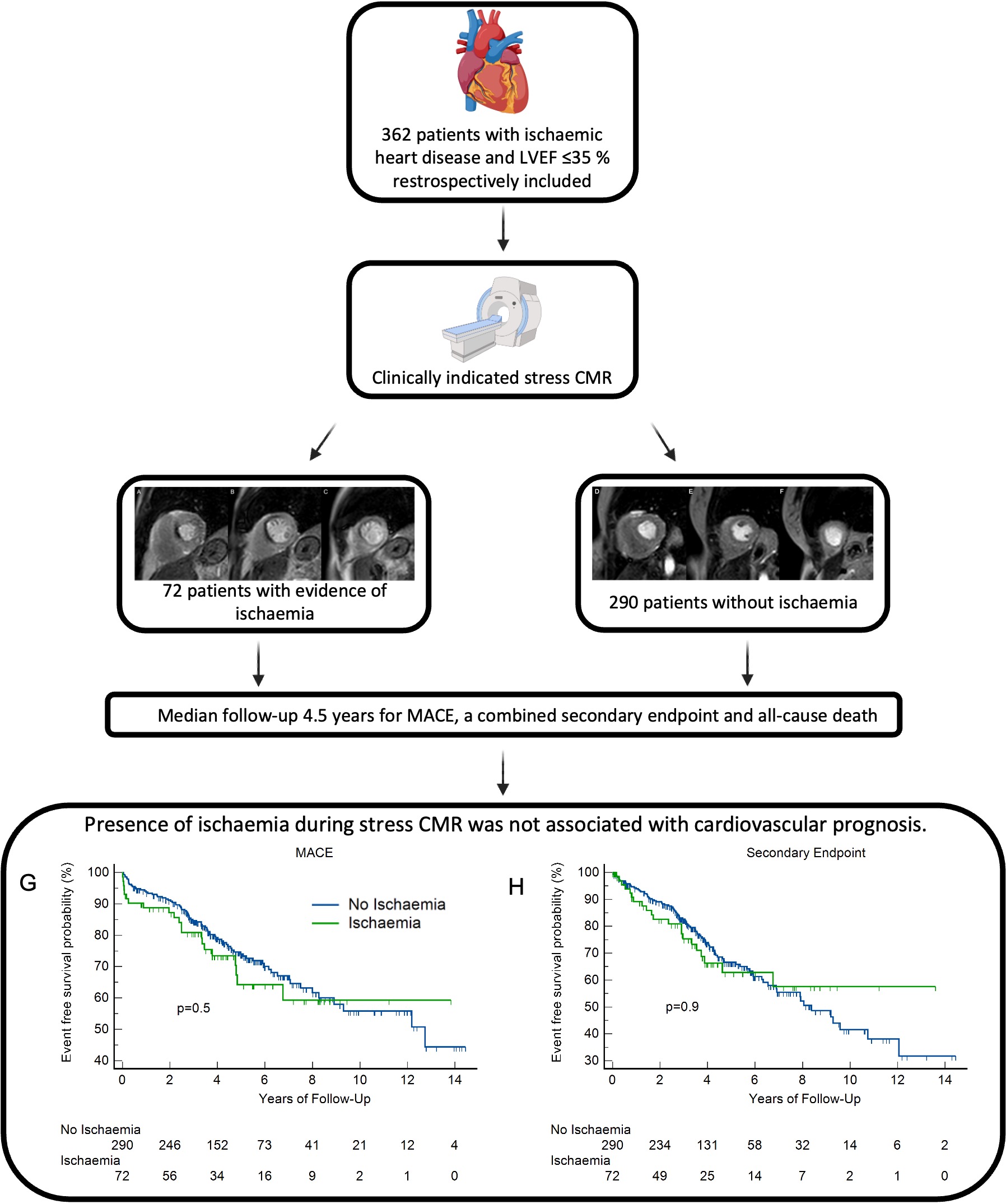
Results: The study population consisted of 362 patients (85.6% men, 70.5 (63.0-78.0) years) with an LVEF of 30.2% (25.2%-33.0%). 245 patients (67.6%) had three vessel disease, 206 patients (57.2%) had a history of MI and 83 patients (22.9%) had a history of CABG. Stress CMR showed ischaemia in 72 (19.9%) patients. Among those, 32 patients (8.8%) underwent early revascularisation. Follow-up was 4.5 (3.0-6.6) years. MACE occurred in 101 patients (27.9%), including 41 cases of cardiac death (11.3%) and 40 cases of MI (11.0%). Ischaemia was not significantly associated with MACE, the combined secondary endpoint, or all-cause death in survival analysis (HR for MACE 1.20, 95% CI 0.74 to 1.95, p=0.4).
Conclusion: In a cohort of patients with IHD and severely reduced LVEF, outcome did not differ when stratifying by ischaemia on stress CMR. We found no evidence that ischaemia could identify patients with increased risk for MACE, the combined secondary endpoint or all-cause death.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


