{"title":"基于MAGGIC风险评分的心衰患者风险分层选择将受益于多学科治疗的患者。","authors":"Yoshiharu Kinugasa, Kensuke Nakamura, Masayuki Hirai, Midori Manba, Natsuko Ishiga, Takeshi Sota, Natsuko Nakayama, Tomoki Ota, Masahiko Kato, Masaru Kato","doi":"10.1136/openhrt-2025-003496","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Guidelines worldwide recommend specialist outpatient clinics staffed by a multidisciplinary team for management of patients with heart failure (HF). However, there is limited information on how best to select these patients for efficient use of resources. This study aimed to determine the effectiveness of team-based care for patients with HF after discharge from hospital according to duration of intervention and stratification of patients according to risk.</p><p><strong>Methods: </strong>We retrospectively identified 185 eligible patients who were hospitalised with acute decompensated HF at our institution between January 2021 and June 2023. Multidisciplinary team care was defined as outpatient follow-up by both cardiologists and nurses postdischarge. The primary outcome was a composite of cardiovascular-related death and readmission with HF within 1 year, which was compared between patients receiving HF team care and those receiving standard follow-up.</p><p><strong>Results: </strong>HF team care was provided for 53.0% of patients, who were younger than those receiving standard follow-up and required more oral inotropes, tolvaptan and amiodarone. Among those receiving HF team care, the majority (58.2%) had an intervention duration of 30 days or less after discharge. After adjusting for background differences by inverse probability of treatment weighting, HF team care was associated with favourable 180-day outcomes, but there was no significant between-group difference in the 1-year primary outcomes. In subgroup analysis, patients with a higher Meta-Analysis Global Group in Chronic Heart Failure score (≥28), indicating a higher risk of exacerbation of HF, had significantly lower 1-year event rates with HF team care (p value for interaction <0.05).</p><p><strong>Conclusions: </strong>Multidisciplinary HF team care is most effective for patients at higher risk of exacerbation of HF. A risk score model may optimise patient selection for specialised care.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406894/pdf/","citationCount":"0","resultStr":"{\"title\":\"MAGGIC risk score-based risk stratification for selecting patients with heart failure who will benefit from multidisciplinary care.\",\"authors\":\"Yoshiharu Kinugasa, Kensuke Nakamura, Masayuki Hirai, Midori Manba, Natsuko Ishiga, Takeshi Sota, Natsuko Nakayama, Tomoki Ota, Masahiko Kato, Masaru Kato\",\"doi\":\"10.1136/openhrt-2025-003496\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Guidelines worldwide recommend specialist outpatient clinics staffed by a multidisciplinary team for management of patients with heart failure (HF). However, there is limited information on how best to select these patients for efficient use of resources. This study aimed to determine the effectiveness of team-based care for patients with HF after discharge from hospital according to duration of intervention and stratification of patients according to risk.</p><p><strong>Methods: </strong>We retrospectively identified 185 eligible patients who were hospitalised with acute decompensated HF at our institution between January 2021 and June 2023. Multidisciplinary team care was defined as outpatient follow-up by both cardiologists and nurses postdischarge. The primary outcome was a composite of cardiovascular-related death and readmission with HF within 1 year, which was compared between patients receiving HF team care and those receiving standard follow-up.</p><p><strong>Results: </strong>HF team care was provided for 53.0% of patients, who were younger than those receiving standard follow-up and required more oral inotropes, tolvaptan and amiodarone. Among those receiving HF team care, the majority (58.2%) had an intervention duration of 30 days or less after discharge. After adjusting for background differences by inverse probability of treatment weighting, HF team care was associated with favourable 180-day outcomes, but there was no significant between-group difference in the 1-year primary outcomes. In subgroup analysis, patients with a higher Meta-Analysis Global Group in Chronic Heart Failure score (≥28), indicating a higher risk of exacerbation of HF, had significantly lower 1-year event rates with HF team care (p value for interaction <0.05).</p><p><strong>Conclusions: </strong>Multidisciplinary HF team care is most effective for patients at higher risk of exacerbation of HF. A risk score model may optimise patient selection for specialised care.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406894/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2025-003496\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003496","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
MAGGIC risk score-based risk stratification for selecting patients with heart failure who will benefit from multidisciplinary care.
Objective: Guidelines worldwide recommend specialist outpatient clinics staffed by a multidisciplinary team for management of patients with heart failure (HF). However, there is limited information on how best to select these patients for efficient use of resources. This study aimed to determine the effectiveness of team-based care for patients with HF after discharge from hospital according to duration of intervention and stratification of patients according to risk.
Methods: We retrospectively identified 185 eligible patients who were hospitalised with acute decompensated HF at our institution between January 2021 and June 2023. Multidisciplinary team care was defined as outpatient follow-up by both cardiologists and nurses postdischarge. The primary outcome was a composite of cardiovascular-related death and readmission with HF within 1 year, which was compared between patients receiving HF team care and those receiving standard follow-up.
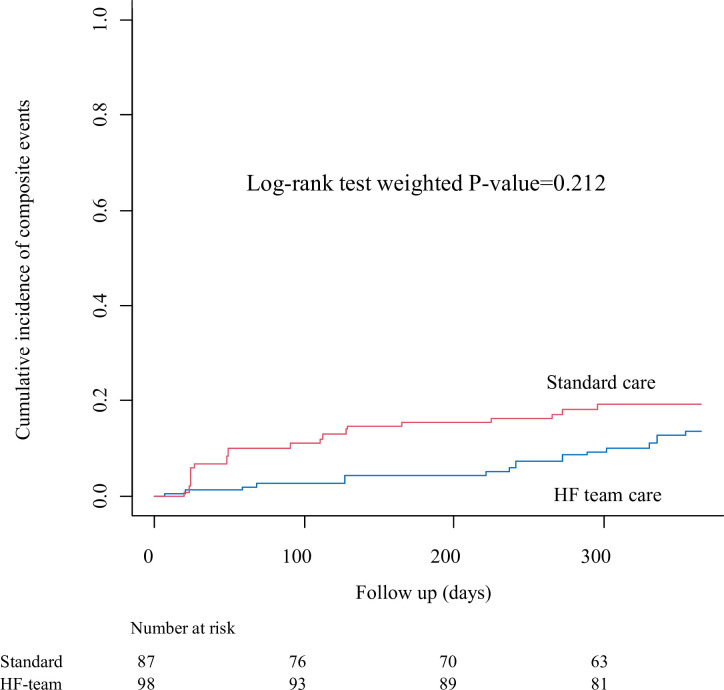
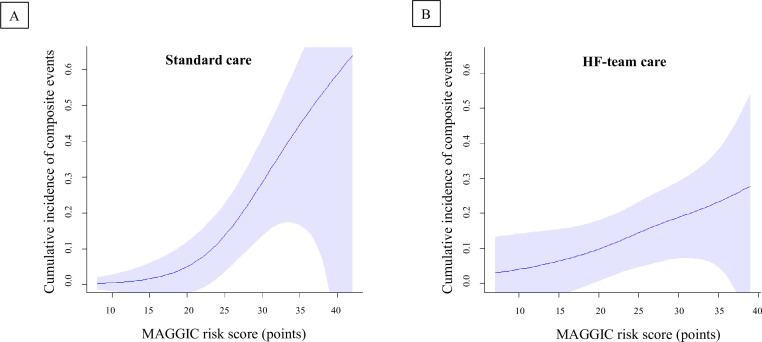
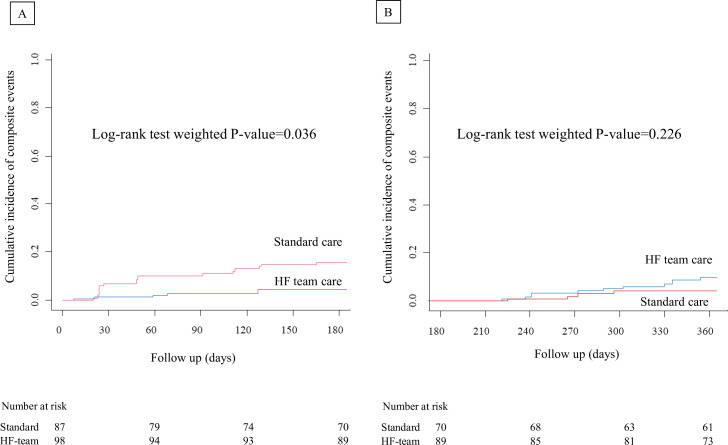
Results: HF team care was provided for 53.0% of patients, who were younger than those receiving standard follow-up and required more oral inotropes, tolvaptan and amiodarone. Among those receiving HF team care, the majority (58.2%) had an intervention duration of 30 days or less after discharge. After adjusting for background differences by inverse probability of treatment weighting, HF team care was associated with favourable 180-day outcomes, but there was no significant between-group difference in the 1-year primary outcomes. In subgroup analysis, patients with a higher Meta-Analysis Global Group in Chronic Heart Failure score (≥28), indicating a higher risk of exacerbation of HF, had significantly lower 1-year event rates with HF team care (p value for interaction <0.05).
Conclusions: Multidisciplinary HF team care is most effective for patients at higher risk of exacerbation of HF. A risk score model may optimise patient selection for specialised care.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


