Anna Bacchetti, Ting-Yi Lin, Brenna McCormack, Omar Ezzedin, Rozita Doosti, Gelareh Ahmadi, Nicole Pellegrini, Evan Johnson, Simidele Davis, Elle Lawrence, Gabriel Otero-Duran, Ernest Lievers, Madeline Inserra, Sooyeon Park, Devon Bonair, Anna Kim, Ananya Gulati, Kathryn C Fitzgerald, Elias S Sotirchos, Peter A Calabresi, Shiv Saidha
{"title":"OSCAR-IB标准对多发性硬化症患者卷云HD-OCT视网膜厚度测量重测信度的影响","authors":"Anna Bacchetti, Ting-Yi Lin, Brenna McCormack, Omar Ezzedin, Rozita Doosti, Gelareh Ahmadi, Nicole Pellegrini, Evan Johnson, Simidele Davis, Elle Lawrence, Gabriel Otero-Duran, Ernest Lievers, Madeline Inserra, Sooyeon Park, Devon Bonair, Anna Kim, Ananya Gulati, Kathryn C Fitzgerald, Elias S Sotirchos, Peter A Calabresi, Shiv Saidha","doi":"10.1212/NXI.0000000000200458","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Optical coherence tomography (OCT) allows evaluation of inter-eye differences (IEDs) in macular ganglion cell-inner plexiform layer (GCIPL) and peripapillary retinal nerve fiber layer (pRNFL) thicknesses to identify unilateral optic nerve involvement (UONI). UONI supports dissemination in space (DIS) as part of the 2024 revised McDonald diagnostic criteria for multiple sclerosis (MS). The OSCAR-IB quality control (QC) criteria identify suboptimal-quality OCT scans, which could potentially result in false-positive or false-negative UONI identification. We aimed to determine the influence of scans fulfilling OSCAR-IB criteria (SFO) and not fulfilling (SNFO) on test-retest reliability of pRNFL and GCIPL thicknesses/IEDs, with a commonly used OCT platform (Cirrus HD-OCT).</p><p><strong>Methods: </strong>A total of 509 participants, including 397 people with MS, underwent Cirrus HD-OCT, with acquisition of 2 macular and optic disc scans per eye. Each scan was classified as either SFO or SNFO. There were no clinical or demographic exclusions in order to reflect a real-world clinical setting. Reproducibility was evaluated with intravisit intraclass correlation coefficients (ICCs) and coefficients of variation (COVs). IED consistency was assessed with difference-in-differences (DiDs) and probabilities of agreement (POA) for specific IED thresholds (GCIPL </≥4; pRNFL </≥6 μm).</p><p><strong>Results: </strong>A total of 1,143 macular scan pairs (1,100 SFO and 42 SNFO) for GCIPL and 1,108 optic disc scan pairs (1,003 SFO and 105 SNFO) for pRNFL were analyzed. SFO demonstrated superior reliability, as compared to SNFO for GCIPL (SFO: ICC = 0.998, COV = 0.40%; SNFO: ICC 0.353, COV 10.14%) and pRNFL (SFO: ICC = 0.989, COV = 1.18%; SNFO: ICC = 0.852, COV = 3.94%) thicknesses. DiDs were lower for SFO (GCIPL 0.64 ± 0.67 μm, pRNFL: 2.00 ± 1.72 μm), as compared to SNFO (GCIPL: 10.17 ± 13.87 μm, pRNFL: 4.78 ± 5.51 μm). POA of IED thresholds (GCIPL: </≥4; pRNFL: </≥6 μm) was higher for SFO than for SNFO (GCIPL: 95.58% vs 47.83%; pRNFL: 86.89% vs 71.67%).</p><p><strong>Discussion: </strong>GCIPL and pRNFL thicknesses/IEDs demonstrated markedly inferior reliability in SNFO, relative to SFO. Failure to fulfill OSCAR-IB criteria influenced pRNFL measurements and, in particular, GCIPL measurements, highlighting the importance of thorough QC in the interpretation of OCT to correctly identify UONI and accurately support DIS for the diagnosis of MS.</p>","PeriodicalId":19472,"journal":{"name":"Neurology® Neuroimmunology & Neuroinflammation","volume":"12 6","pages":"e200458"},"PeriodicalIF":7.5000,"publicationDate":"2025-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401565/pdf/","citationCount":"0","resultStr":"{\"title\":\"Influence of OSCAR-IB Criteria on Test-Retest Reliability of Cirrus HD-OCT Retinal Thickness Measurements in People With Multiple Sclerosis.\",\"authors\":\"Anna Bacchetti, Ting-Yi Lin, Brenna McCormack, Omar Ezzedin, Rozita Doosti, Gelareh Ahmadi, Nicole Pellegrini, Evan Johnson, Simidele Davis, Elle Lawrence, Gabriel Otero-Duran, Ernest Lievers, Madeline Inserra, Sooyeon Park, Devon Bonair, Anna Kim, Ananya Gulati, Kathryn C Fitzgerald, Elias S Sotirchos, Peter A Calabresi, Shiv Saidha\",\"doi\":\"10.1212/NXI.0000000000200458\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Optical coherence tomography (OCT) allows evaluation of inter-eye differences (IEDs) in macular ganglion cell-inner plexiform layer (GCIPL) and peripapillary retinal nerve fiber layer (pRNFL) thicknesses to identify unilateral optic nerve involvement (UONI). UONI supports dissemination in space (DIS) as part of the 2024 revised McDonald diagnostic criteria for multiple sclerosis (MS). The OSCAR-IB quality control (QC) criteria identify suboptimal-quality OCT scans, which could potentially result in false-positive or false-negative UONI identification. We aimed to determine the influence of scans fulfilling OSCAR-IB criteria (SFO) and not fulfilling (SNFO) on test-retest reliability of pRNFL and GCIPL thicknesses/IEDs, with a commonly used OCT platform (Cirrus HD-OCT).</p><p><strong>Methods: </strong>A total of 509 participants, including 397 people with MS, underwent Cirrus HD-OCT, with acquisition of 2 macular and optic disc scans per eye. Each scan was classified as either SFO or SNFO. There were no clinical or demographic exclusions in order to reflect a real-world clinical setting. Reproducibility was evaluated with intravisit intraclass correlation coefficients (ICCs) and coefficients of variation (COVs). IED consistency was assessed with difference-in-differences (DiDs) and probabilities of agreement (POA) for specific IED thresholds (GCIPL </≥4; pRNFL </≥6 μm).</p><p><strong>Results: </strong>A total of 1,143 macular scan pairs (1,100 SFO and 42 SNFO) for GCIPL and 1,108 optic disc scan pairs (1,003 SFO and 105 SNFO) for pRNFL were analyzed. SFO demonstrated superior reliability, as compared to SNFO for GCIPL (SFO: ICC = 0.998, COV = 0.40%; SNFO: ICC 0.353, COV 10.14%) and pRNFL (SFO: ICC = 0.989, COV = 1.18%; SNFO: ICC = 0.852, COV = 3.94%) thicknesses. DiDs were lower for SFO (GCIPL 0.64 ± 0.67 μm, pRNFL: 2.00 ± 1.72 μm), as compared to SNFO (GCIPL: 10.17 ± 13.87 μm, pRNFL: 4.78 ± 5.51 μm). POA of IED thresholds (GCIPL: </≥4; pRNFL: </≥6 μm) was higher for SFO than for SNFO (GCIPL: 95.58% vs 47.83%; pRNFL: 86.89% vs 71.67%).</p><p><strong>Discussion: </strong>GCIPL and pRNFL thicknesses/IEDs demonstrated markedly inferior reliability in SNFO, relative to SFO. Failure to fulfill OSCAR-IB criteria influenced pRNFL measurements and, in particular, GCIPL measurements, highlighting the importance of thorough QC in the interpretation of OCT to correctly identify UONI and accurately support DIS for the diagnosis of MS.</p>\",\"PeriodicalId\":19472,\"journal\":{\"name\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"volume\":\"12 6\",\"pages\":\"e200458\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2025-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401565/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000200458\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology® Neuroimmunology & Neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200458","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Influence of OSCAR-IB Criteria on Test-Retest Reliability of Cirrus HD-OCT Retinal Thickness Measurements in People With Multiple Sclerosis.
Background and objectives: Optical coherence tomography (OCT) allows evaluation of inter-eye differences (IEDs) in macular ganglion cell-inner plexiform layer (GCIPL) and peripapillary retinal nerve fiber layer (pRNFL) thicknesses to identify unilateral optic nerve involvement (UONI). UONI supports dissemination in space (DIS) as part of the 2024 revised McDonald diagnostic criteria for multiple sclerosis (MS). The OSCAR-IB quality control (QC) criteria identify suboptimal-quality OCT scans, which could potentially result in false-positive or false-negative UONI identification. We aimed to determine the influence of scans fulfilling OSCAR-IB criteria (SFO) and not fulfilling (SNFO) on test-retest reliability of pRNFL and GCIPL thicknesses/IEDs, with a commonly used OCT platform (Cirrus HD-OCT).
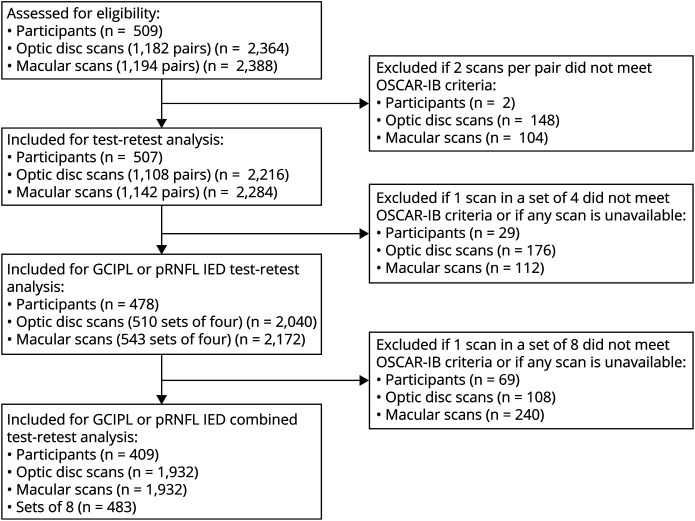
Methods: A total of 509 participants, including 397 people with MS, underwent Cirrus HD-OCT, with acquisition of 2 macular and optic disc scans per eye. Each scan was classified as either SFO or SNFO. There were no clinical or demographic exclusions in order to reflect a real-world clinical setting. Reproducibility was evaluated with intravisit intraclass correlation coefficients (ICCs) and coefficients of variation (COVs). IED consistency was assessed with difference-in-differences (DiDs) and probabilities of agreement (POA) for specific IED thresholds (GCIPL
Results: A total of 1,143 macular scan pairs (1,100 SFO and 42 SNFO) for GCIPL and 1,108 optic disc scan pairs (1,003 SFO and 105 SNFO) for pRNFL were analyzed. SFO demonstrated superior reliability, as compared to SNFO for GCIPL (SFO: ICC = 0.998, COV = 0.40%; SNFO: ICC 0.353, COV 10.14%) and pRNFL (SFO: ICC = 0.989, COV = 1.18%; SNFO: ICC = 0.852, COV = 3.94%) thicknesses. DiDs were lower for SFO (GCIPL 0.64 ± 0.67 μm, pRNFL: 2.00 ± 1.72 μm), as compared to SNFO (GCIPL: 10.17 ± 13.87 μm, pRNFL: 4.78 ± 5.51 μm). POA of IED thresholds (GCIPL:
Discussion: GCIPL and pRNFL thicknesses/IEDs demonstrated markedly inferior reliability in SNFO, relative to SFO. Failure to fulfill OSCAR-IB criteria influenced pRNFL measurements and, in particular, GCIPL measurements, highlighting the importance of thorough QC in the interpretation of OCT to correctly identify UONI and accurately support DIS for the diagnosis of MS.
期刊介绍:
Neurology Neuroimmunology & Neuroinflammation is an official journal of the American Academy of Neurology. Neurology: Neuroimmunology & Neuroinflammation will be the premier peer-reviewed journal in neuroimmunology and neuroinflammation. This journal publishes rigorously peer-reviewed open-access reports of original research and in-depth reviews of topics in neuroimmunology & neuroinflammation, affecting the full range of neurologic diseases including (but not limited to) Alzheimer's disease, Parkinson's disease, ALS, tauopathy, and stroke; multiple sclerosis and NMO; inflammatory peripheral nerve and muscle disease, Guillain-Barré and myasthenia gravis; nervous system infection; paraneoplastic syndromes, noninfectious encephalitides and other antibody-mediated disorders; and psychiatric and neurodevelopmental disorders. Clinical trials, instructive case reports, and small case series will also be featured.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


