Lalanthica V Yogendran, Abhinav Kareddy, Salma O Abbas, Zachary Scharf, James Patrie, Sohil H Patel, David Schiff
{"title":"替莫唑胺对2/3级IDH突变胶质瘤首次进展的影响。","authors":"Lalanthica V Yogendran, Abhinav Kareddy, Salma O Abbas, Zachary Scharf, James Patrie, Sohil H Patel, David Schiff","doi":"10.1007/s11060-025-05087-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with WHO grade 2 and 3 isocitrate dehydrogenase mutation (IDHmt) gliomas commonly receive temozolomide (TMZ), with or without radiation therapy, as initial therapy. At progression, TMZ is sometimes reinstated despite a paucity of data on effectiveness.</p><p><strong>Methods: </strong>We reviewed imaging outcomes of patients with WHO 2016 grade II/III IDHmt gliomas re-treated with TMZ at first progression between 2007 and 2019. Tumor growth rates were calculated over the year preceding re-treatment and throughout the re-treatment period, ranging from 3 to 41 months. RANO criteria were utilized to assess TMZ response rate.</p><p><strong>Results: </strong>15 subjects included six grade II, five grade III oligodendrogliomas, one grade II and three grade III astrocytomas. Median time between completion of the first TMZ course and initiation of re-treatment was 47 months. Median progression-free survival with TMZ re-treatment was 27.4 months and median overall survival was 47.8 months. Mean rate of tumor growth by bidimensional product increased from 0.29 cm<sup>2</sup> /month, in the year prior to first tumor progression, to 0.47 cm<sup>2</sup>/month during re-treatment, ranging from 3 to 41 months, with monotherapy TMZ. Volumetric mean rate of tumor growth was 1.12 cc/month in the year prior to first tumor progression versus 1.29 cc/month during TMZ re-treatment. Five patients experienced tumor growth rate reduction, of whom 3 patients experienced tumor shrinkage as measured by 2D; 2 of these 3 patients also experienced tumor shrinkage as measured by 3D. There was no radiographic response by RANO criteria.</p><p><strong>Conclusion: </strong>These findings suggest previously treated, progressive IDHmt gliomas are generally resistant to TMZ, underscoring the need for alternative approaches.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"1147-1154"},"PeriodicalIF":3.1000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12511160/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of re-challenge with temozolomide in grade 2/3 IDH mutant gliomas at first progression.\",\"authors\":\"Lalanthica V Yogendran, Abhinav Kareddy, Salma O Abbas, Zachary Scharf, James Patrie, Sohil H Patel, David Schiff\",\"doi\":\"10.1007/s11060-025-05087-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with WHO grade 2 and 3 isocitrate dehydrogenase mutation (IDHmt) gliomas commonly receive temozolomide (TMZ), with or without radiation therapy, as initial therapy. At progression, TMZ is sometimes reinstated despite a paucity of data on effectiveness.</p><p><strong>Methods: </strong>We reviewed imaging outcomes of patients with WHO 2016 grade II/III IDHmt gliomas re-treated with TMZ at first progression between 2007 and 2019. Tumor growth rates were calculated over the year preceding re-treatment and throughout the re-treatment period, ranging from 3 to 41 months. RANO criteria were utilized to assess TMZ response rate.</p><p><strong>Results: </strong>15 subjects included six grade II, five grade III oligodendrogliomas, one grade II and three grade III astrocytomas. Median time between completion of the first TMZ course and initiation of re-treatment was 47 months. Median progression-free survival with TMZ re-treatment was 27.4 months and median overall survival was 47.8 months. Mean rate of tumor growth by bidimensional product increased from 0.29 cm<sup>2</sup> /month, in the year prior to first tumor progression, to 0.47 cm<sup>2</sup>/month during re-treatment, ranging from 3 to 41 months, with monotherapy TMZ. Volumetric mean rate of tumor growth was 1.12 cc/month in the year prior to first tumor progression versus 1.29 cc/month during TMZ re-treatment. Five patients experienced tumor growth rate reduction, of whom 3 patients experienced tumor shrinkage as measured by 2D; 2 of these 3 patients also experienced tumor shrinkage as measured by 3D. There was no radiographic response by RANO criteria.</p><p><strong>Conclusion: </strong>These findings suggest previously treated, progressive IDHmt gliomas are generally resistant to TMZ, underscoring the need for alternative approaches.</p>\",\"PeriodicalId\":16425,\"journal\":{\"name\":\"Journal of Neuro-Oncology\",\"volume\":\" \",\"pages\":\"1147-1154\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12511160/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neuro-Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11060-025-05087-w\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-025-05087-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Effects of re-challenge with temozolomide in grade 2/3 IDH mutant gliomas at first progression.
Background: Patients with WHO grade 2 and 3 isocitrate dehydrogenase mutation (IDHmt) gliomas commonly receive temozolomide (TMZ), with or without radiation therapy, as initial therapy. At progression, TMZ is sometimes reinstated despite a paucity of data on effectiveness.
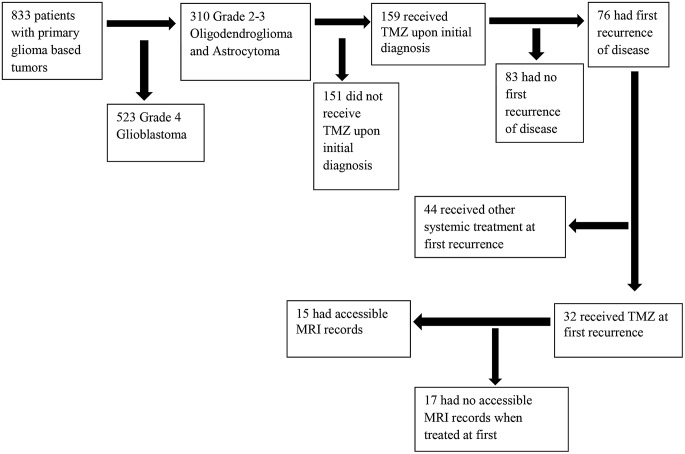
Methods: We reviewed imaging outcomes of patients with WHO 2016 grade II/III IDHmt gliomas re-treated with TMZ at first progression between 2007 and 2019. Tumor growth rates were calculated over the year preceding re-treatment and throughout the re-treatment period, ranging from 3 to 41 months. RANO criteria were utilized to assess TMZ response rate.
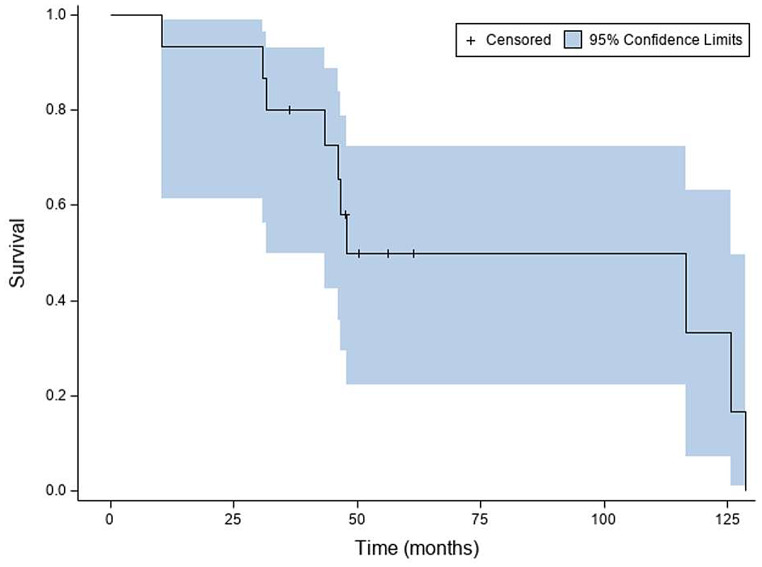
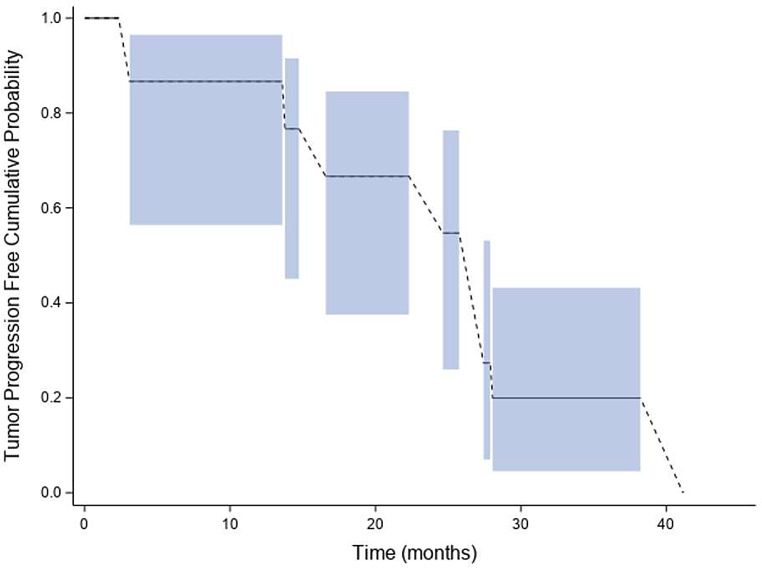
Results: 15 subjects included six grade II, five grade III oligodendrogliomas, one grade II and three grade III astrocytomas. Median time between completion of the first TMZ course and initiation of re-treatment was 47 months. Median progression-free survival with TMZ re-treatment was 27.4 months and median overall survival was 47.8 months. Mean rate of tumor growth by bidimensional product increased from 0.29 cm2 /month, in the year prior to first tumor progression, to 0.47 cm2/month during re-treatment, ranging from 3 to 41 months, with monotherapy TMZ. Volumetric mean rate of tumor growth was 1.12 cc/month in the year prior to first tumor progression versus 1.29 cc/month during TMZ re-treatment. Five patients experienced tumor growth rate reduction, of whom 3 patients experienced tumor shrinkage as measured by 2D; 2 of these 3 patients also experienced tumor shrinkage as measured by 3D. There was no radiographic response by RANO criteria.
Conclusion: These findings suggest previously treated, progressive IDHmt gliomas are generally resistant to TMZ, underscoring the need for alternative approaches.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


