David Waterhouse, Iris Li, Laura Morrison, Bruno Emond, Marie-Hélène Lafeuille, Annalise Hilts, Jill Korsiak, Patrick Lefebvre, Pratyusha Vadagam, Dexter Waters
{"title":"egfr突变晚期或转移性非小细胞肺癌患者的医疗资源使用、医疗费用和未满足需求","authors":"David Waterhouse, Iris Li, Laura Morrison, Bruno Emond, Marie-Hélène Lafeuille, Annalise Hilts, Jill Korsiak, Patrick Lefebvre, Pratyusha Vadagam, Dexter Waters","doi":"10.36469/001c.142771","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Approximately 17% of patients with non-small cell lung cancer (NSCLC) have epidermal growth factor receptor-mutated (EGFRm) NSCLC, 84% of which are exon 19 deletions (Ex19del)/exon 21 substitutions (L858R). Unmet needs for patients treated with tyrosine kinase inhibitors (TKIs) for EGFRm (Ex19del/L858R) advanced NSCLC, including osimertinib, are relevant to US population health decision makers.</p><p><strong>Objectives: </strong>To describe healthcare resource utilization (HRU) and costs by line of therapy (LOT) among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating first-line (1L) treatment.</p><p><strong>Methods: </strong>IBM MarketScan® Research Databases (1/1/2010-1/31/2023) were used to select adult patients with advanced NSCLC initiating an EGFR-TKI during any LOT on/after 4/18/2018 (osimertinib approval; EGFRm Ex19del/L858R proxy). Per-patient-per-month (PPPM) all-cause HRU and costs were described in 1L, second-line (2L), and third-line (3L) overall and among subgroups receiving 1L osimertinib monotherapy or platinum-based chemotherapy (PBC) without immunotherapy, separately.</p><p><strong>Results: </strong>The study included 409 patients with EGFRm advanced NSCLC (mean age, 60.5 years; 70.2% female). In 1L, 72.9% initiated osimertinib-based therapy (2L, 45.9%; 3L, 41.2%), 21.0% initiated chemotherapy (2L, 30.0%; 3L, 36.5%), 4.6% initiated another EGFR-TKI (2L, 12.9%; 3L, 12.9%), and 1.5% initiated immunotherapy (2L, 11.2%; 3L, 9.4%). Overall, 170 patients (41.6%) progressed to 2L among whom 85 (50.0%) progressed to 3L. Mean LOT duration decreased with each successive LOT (1L, 10.2 months; 2L, 8.7 months; 3L, 8.0 months). Across LOTs, patients had a mean of >4 outpatient visits PPPM (1L, 4.79; 2L, 4.26; 3L, 4.40), and the 1L osimertinib monotherapy subgroup (n = 279) had a mean of 0.69 inpatient days PPPM during 1L (2L, 0.82; 3L, 0.74). Mean all-cause costs PPPM were <math><mn>27</mn> <mrow><mo> </mo></mrow> <mn>751</mn> <mi>i</mi> <mi>n</mi> <mn>1</mn> <mi>L</mi> <mo>,</mo></math> 28 971 in 2L, and <math><mn>31</mn> <mrow><mo> </mo></mrow> <mn>251</mn> <mi>i</mi> <mi>n</mi> <mn>3</mn> <mi>L</mi> <mo>.</mo> <mi>A</mi> <mi>m</mi> <mi>o</mi> <mi>n</mi> <mi>g</mi> <mi>t</mi> <mi>h</mi> <mi>e</mi> <mn>1</mn> <mi>L</mi> <mi>o</mi> <mi>s</mi> <mi>i</mi> <mi>m</mi> <mi>e</mi> <mi>r</mi> <mi>t</mi> <mi>i</mi> <mi>n</mi> <mi>i</mi> <mi>b</mi> <mi>m</mi> <mi>o</mi> <mi>n</mi> <mi>o</mi> <mi>t</mi> <mi>h</mi> <mi>e</mi> <mi>r</mi> <mi>a</mi> <mi>p</mi> <mi>y</mi> <mi>s</mi> <mi>u</mi> <mi>b</mi> <mi>g</mi> <mi>r</mi> <mi>o</mi> <mi>u</mi> <mi>p</mi> <mo>,</mo> <mi>m</mi> <mi>e</mi> <mi>a</mi> <mi>n</mi> <mi>P</mi> <mi>P</mi> <mi>P</mi> <mi>M</mi> <mi>c</mi> <mi>o</mi> <mi>s</mi> <mi>t</mi> <mi>s</mi> <mi>w</mi> <mi>e</mi> <mi>r</mi> <mi>e</mi></math> 27 610 in 1L, <math><mn>35</mn> <mrow><mo> </mo></mrow> <mn>501</mn> <mi>i</mi> <mi>n</mi> <mn>2</mn> <mi>L</mi> <mo>,</mo> <mi>a</mi> <mi>n</mi> <mi>d</mi></math> 36 618 in 3L. Among the 1L PBC subgroup (n = 58), mean PPPM costs were <math><mn>23</mn> <mrow><mo> </mo></mrow> <mn>820</mn> <mi>i</mi> <mi>n</mi> <mn>1</mn> <mi>L</mi> <mo>,</mo></math> 24 788 in 2L, and $23 348 in 3L.</p><p><strong>Discussion: </strong>Among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating 1L, each successive LOT was shorter and more costly.</p><p><strong>Conclusions: </strong>Findings highlight the importance of using the most effective 1L treatments to delay disease progression and reduce HRU and costs.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 2","pages":"98-107"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399230/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare Resource Use, Healthcare Costs, and Unmet Needs Among Patients Treated for EGFR-Mutated Advanced or Metastatic Non-small Cell Lung Cancer.\",\"authors\":\"David Waterhouse, Iris Li, Laura Morrison, Bruno Emond, Marie-Hélène Lafeuille, Annalise Hilts, Jill Korsiak, Patrick Lefebvre, Pratyusha Vadagam, Dexter Waters\",\"doi\":\"10.36469/001c.142771\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Approximately 17% of patients with non-small cell lung cancer (NSCLC) have epidermal growth factor receptor-mutated (EGFRm) NSCLC, 84% of which are exon 19 deletions (Ex19del)/exon 21 substitutions (L858R). Unmet needs for patients treated with tyrosine kinase inhibitors (TKIs) for EGFRm (Ex19del/L858R) advanced NSCLC, including osimertinib, are relevant to US population health decision makers.</p><p><strong>Objectives: </strong>To describe healthcare resource utilization (HRU) and costs by line of therapy (LOT) among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating first-line (1L) treatment.</p><p><strong>Methods: </strong>IBM MarketScan® Research Databases (1/1/2010-1/31/2023) were used to select adult patients with advanced NSCLC initiating an EGFR-TKI during any LOT on/after 4/18/2018 (osimertinib approval; EGFRm Ex19del/L858R proxy). Per-patient-per-month (PPPM) all-cause HRU and costs were described in 1L, second-line (2L), and third-line (3L) overall and among subgroups receiving 1L osimertinib monotherapy or platinum-based chemotherapy (PBC) without immunotherapy, separately.</p><p><strong>Results: </strong>The study included 409 patients with EGFRm advanced NSCLC (mean age, 60.5 years; 70.2% female). In 1L, 72.9% initiated osimertinib-based therapy (2L, 45.9%; 3L, 41.2%), 21.0% initiated chemotherapy (2L, 30.0%; 3L, 36.5%), 4.6% initiated another EGFR-TKI (2L, 12.9%; 3L, 12.9%), and 1.5% initiated immunotherapy (2L, 11.2%; 3L, 9.4%). Overall, 170 patients (41.6%) progressed to 2L among whom 85 (50.0%) progressed to 3L. Mean LOT duration decreased with each successive LOT (1L, 10.2 months; 2L, 8.7 months; 3L, 8.0 months). Across LOTs, patients had a mean of >4 outpatient visits PPPM (1L, 4.79; 2L, 4.26; 3L, 4.40), and the 1L osimertinib monotherapy subgroup (n = 279) had a mean of 0.69 inpatient days PPPM during 1L (2L, 0.82; 3L, 0.74). Mean all-cause costs PPPM were <math><mn>27</mn> <mrow><mo> </mo></mrow> <mn>751</mn> <mi>i</mi> <mi>n</mi> <mn>1</mn> <mi>L</mi> <mo>,</mo></math> 28 971 in 2L, and <math><mn>31</mn> <mrow><mo> </mo></mrow> <mn>251</mn> <mi>i</mi> <mi>n</mi> <mn>3</mn> <mi>L</mi> <mo>.</mo> <mi>A</mi> <mi>m</mi> <mi>o</mi> <mi>n</mi> <mi>g</mi> <mi>t</mi> <mi>h</mi> <mi>e</mi> <mn>1</mn> <mi>L</mi> <mi>o</mi> <mi>s</mi> <mi>i</mi> <mi>m</mi> <mi>e</mi> <mi>r</mi> <mi>t</mi> <mi>i</mi> <mi>n</mi> <mi>i</mi> <mi>b</mi> <mi>m</mi> <mi>o</mi> <mi>n</mi> <mi>o</mi> <mi>t</mi> <mi>h</mi> <mi>e</mi> <mi>r</mi> <mi>a</mi> <mi>p</mi> <mi>y</mi> <mi>s</mi> <mi>u</mi> <mi>b</mi> <mi>g</mi> <mi>r</mi> <mi>o</mi> <mi>u</mi> <mi>p</mi> <mo>,</mo> <mi>m</mi> <mi>e</mi> <mi>a</mi> <mi>n</mi> <mi>P</mi> <mi>P</mi> <mi>P</mi> <mi>M</mi> <mi>c</mi> <mi>o</mi> <mi>s</mi> <mi>t</mi> <mi>s</mi> <mi>w</mi> <mi>e</mi> <mi>r</mi> <mi>e</mi></math> 27 610 in 1L, <math><mn>35</mn> <mrow><mo> </mo></mrow> <mn>501</mn> <mi>i</mi> <mi>n</mi> <mn>2</mn> <mi>L</mi> <mo>,</mo> <mi>a</mi> <mi>n</mi> <mi>d</mi></math> 36 618 in 3L. Among the 1L PBC subgroup (n = 58), mean PPPM costs were <math><mn>23</mn> <mrow><mo> </mo></mrow> <mn>820</mn> <mi>i</mi> <mi>n</mi> <mn>1</mn> <mi>L</mi> <mo>,</mo></math> 24 788 in 2L, and $23 348 in 3L.</p><p><strong>Discussion: </strong>Among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating 1L, each successive LOT was shorter and more costly.</p><p><strong>Conclusions: </strong>Findings highlight the importance of using the most effective 1L treatments to delay disease progression and reduce HRU and costs.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"12 2\",\"pages\":\"98-107\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399230/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36469/001c.142771\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.142771","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:约17%的非小细胞肺癌(NSCLC)患者为表皮生长因子受体突变(EGFRm)型NSCLC,其中84%为外显子19缺失(Ex19del)/外显子21替换(L858R)。EGFRm (Ex19del/L858R)晚期NSCLC患者未满足的酪氨酸激酶抑制剂(TKIs)治疗需求,包括奥西替尼,与美国人口健康决策者相关。目的:描述EGFRm (Ex19del/L858R)晚期NSCLC患者开始一线(1L)治疗的医疗资源利用率(HRU)和费用(LOT)。方法:使用IBM MarketScan®研究数据库(2010年1月1日- 2023年1月31日)选择2018年4月18日/之后任何LOT期间启动EGFR-TKI的晚期NSCLC成年患者(奥西替尼批准;EGFRm Ex19del/L858R代理)。每个患者每月(PPPM)的全因HRU和成本分别在1L、二线(2L)和三线(3L)总体上和接受1L奥西替尼单药治疗或铂基化疗(PBC)不进行免疫治疗的亚组中进行描述。结果:该研究纳入409例EGFRm晚期NSCLC患者(平均年龄60.5岁,70.2%为女性)。在1L中,72.9%的患者开始了基于奥西替尼的治疗(2L, 45.9%; 3L, 41.2%), 21.0%的患者开始了化疗(2L, 30.0%; 3L, 36.5%), 4.6%的患者开始了另一种EGFR-TKI (2L, 12.9%; 3L, 12.9%), 1.5%的患者开始了免疫治疗(2L, 11.2%; 3L, 9.4%)。总体而言,170例(41.6%)进展为2L,其中85例(50.0%)进展为3L。平均LOT持续时间随每次LOT的延长而减少(1L, 10.2个月;2L, 8.7个月;3L, 8.0个月)。在所有批次中,患者的平均门诊次数PPPM为4840次(1L, 4.79; 2L, 4.26; 3L, 4.40), 1L单药治疗亚组(n = 279)在1L期间的平均住院天数PPPM为0.69天(2L, 0.82; 3L, 0.74)。平均全因成本PPPM为27 751 i / 1 L, 28 971 / 2L, 31 251 / 3 L。m o n g t h e 1 L o s i m e r t i n i b m o n o t h e r p y s u b g r o p m e n p p p m c o s t s w e r e 27 610年1 L,我35 501 n 2 L, n d 36 618 3 L。在1L PBC亚组(n = 58)中,1L的平均PPPM成本为23 820美元,2L为24 788美元,3L为23 348美元。讨论:在EGFRm (Ex19del/L858R)晚期NSCLC患者中,每次连续LOT的时间更短,费用更高。结论:研究结果强调了使用最有效的1L治疗来延缓疾病进展、降低HRU和成本的重要性。
Healthcare Resource Use, Healthcare Costs, and Unmet Needs Among Patients Treated for EGFR-Mutated Advanced or Metastatic Non-small Cell Lung Cancer.
Background: Approximately 17% of patients with non-small cell lung cancer (NSCLC) have epidermal growth factor receptor-mutated (EGFRm) NSCLC, 84% of which are exon 19 deletions (Ex19del)/exon 21 substitutions (L858R). Unmet needs for patients treated with tyrosine kinase inhibitors (TKIs) for EGFRm (Ex19del/L858R) advanced NSCLC, including osimertinib, are relevant to US population health decision makers.
Objectives: To describe healthcare resource utilization (HRU) and costs by line of therapy (LOT) among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating first-line (1L) treatment.
Methods: IBM MarketScan® Research Databases (1/1/2010-1/31/2023) were used to select adult patients with advanced NSCLC initiating an EGFR-TKI during any LOT on/after 4/18/2018 (osimertinib approval; EGFRm Ex19del/L858R proxy). Per-patient-per-month (PPPM) all-cause HRU and costs were described in 1L, second-line (2L), and third-line (3L) overall and among subgroups receiving 1L osimertinib monotherapy or platinum-based chemotherapy (PBC) without immunotherapy, separately.
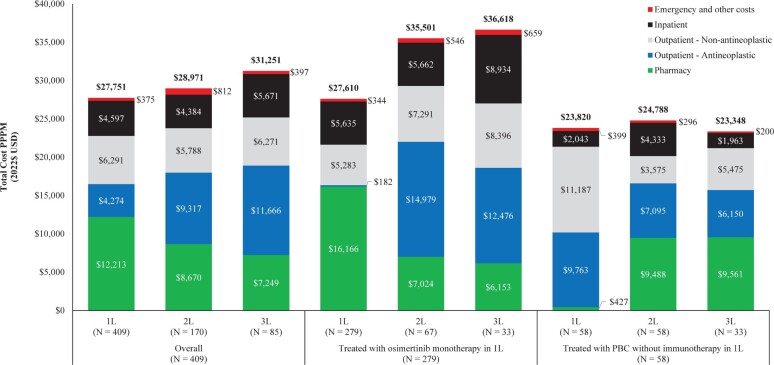
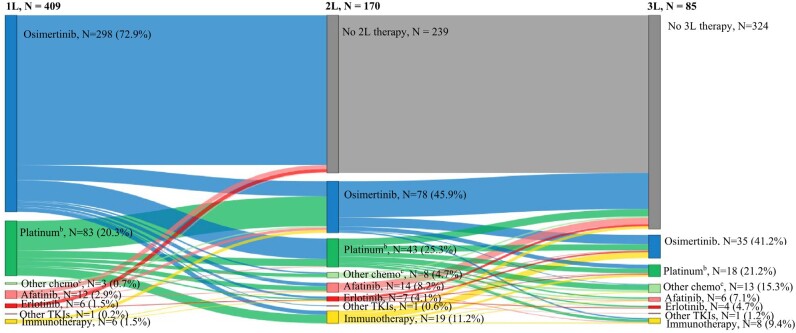
Results: The study included 409 patients with EGFRm advanced NSCLC (mean age, 60.5 years; 70.2% female). In 1L, 72.9% initiated osimertinib-based therapy (2L, 45.9%; 3L, 41.2%), 21.0% initiated chemotherapy (2L, 30.0%; 3L, 36.5%), 4.6% initiated another EGFR-TKI (2L, 12.9%; 3L, 12.9%), and 1.5% initiated immunotherapy (2L, 11.2%; 3L, 9.4%). Overall, 170 patients (41.6%) progressed to 2L among whom 85 (50.0%) progressed to 3L. Mean LOT duration decreased with each successive LOT (1L, 10.2 months; 2L, 8.7 months; 3L, 8.0 months). Across LOTs, patients had a mean of >4 outpatient visits PPPM (1L, 4.79; 2L, 4.26; 3L, 4.40), and the 1L osimertinib monotherapy subgroup (n = 279) had a mean of 0.69 inpatient days PPPM during 1L (2L, 0.82; 3L, 0.74). Mean all-cause costs PPPM were 28 971 in 2L, and 27 610 in 1L, 36 618 in 3L. Among the 1L PBC subgroup (n = 58), mean PPPM costs were 24 788 in 2L, and $23 348 in 3L.
Discussion: Among patients with EGFRm (Ex19del/L858R) advanced NSCLC initiating 1L, each successive LOT was shorter and more costly.
Conclusions: Findings highlight the importance of using the most effective 1L treatments to delay disease progression and reduce HRU and costs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


