{"title":"主动脉夹层的延迟诊断:胸片上被忽视的线索。","authors":"Yao Chen, Wenjin Wang, Lian Lin, Zhankai Tang","doi":"10.1186/s12245-025-00971-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute aortic dissection (AD) is a life-threatening vascular emergency requiring immediate intervention, with mortality rates increasing by 1-2% per hour post-onset. The pathophysiology involves an intimal tear that permits blood to enter the medial layer, forming a false lumen that may expand and compromise branch vessels and end-organ perfusion. Current guidelines from the European Society of Cardiology (ESC), American College of Cardiology (ACC), and American Heart Association (AHA) highlight the necessity of risk stratification based on clinical features (e.g., tearing pain, pulse deficits), predisposing factors (e.g., hypertension), and D-dimer levels, followed by confirmatory imaging with transthoracic echocardiography (TTE) or computed tomography angiography (CTA). Despite advancements in imaging, chest radiography (CXR) remains underutilized; however, key findings-such as mediastinal widening (≥ 5 cm at the aortic knob), abnormal aortic contour, and displaced intimal calcifications-can offer critical diagnostic information.</p><p><strong>Case report: </strong>A young male patient presented with acute chest pain following strenuous exertion. Initial outpatient evaluation, including complete blood count (CBC), liver function tests (LFTs), renal function tests (RFTs), cardiac enzymes, and chest X-ray (CXR), yielded nondiagnostic results, leading to his discharge with analgesics. Three days later, during a national holiday when outpatient clinics were closed, the patient returned to the emergency department (ED) with persistent chest pain. A meticulous review of the initial CXR by the emergency physician revealed mediastinal widening (measuring 8.5 cm) and an abnormal contour of the aorta. Subsequent emergency computed tomography angiography (CTA) confirmed the diagnosis of a Stanford type B aortic dissection.</p><p><strong>Conclusions: </strong>This case underscores two critical learning points: (1) the diagnostic pitfalls associated with atypical early presentations of aortic dissection, and (2) the often underappreciated value of meticulous interpretation of chest X-rays in the evaluation of acute chest pain, particularly when initial studies yield unremarkable results. The three-day diagnostic delay emphasizes the necessity of maintaining a high index of suspicion for aortic dissection, even in young patients lacking classic risk factors.</p>","PeriodicalId":13967,"journal":{"name":"International Journal of Emergency Medicine","volume":"18 1","pages":"158"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382138/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed diagnosis of aortic dissection: the overlooked clues on chest X-ray.\",\"authors\":\"Yao Chen, Wenjin Wang, Lian Lin, Zhankai Tang\",\"doi\":\"10.1186/s12245-025-00971-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute aortic dissection (AD) is a life-threatening vascular emergency requiring immediate intervention, with mortality rates increasing by 1-2% per hour post-onset. The pathophysiology involves an intimal tear that permits blood to enter the medial layer, forming a false lumen that may expand and compromise branch vessels and end-organ perfusion. Current guidelines from the European Society of Cardiology (ESC), American College of Cardiology (ACC), and American Heart Association (AHA) highlight the necessity of risk stratification based on clinical features (e.g., tearing pain, pulse deficits), predisposing factors (e.g., hypertension), and D-dimer levels, followed by confirmatory imaging with transthoracic echocardiography (TTE) or computed tomography angiography (CTA). Despite advancements in imaging, chest radiography (CXR) remains underutilized; however, key findings-such as mediastinal widening (≥ 5 cm at the aortic knob), abnormal aortic contour, and displaced intimal calcifications-can offer critical diagnostic information.</p><p><strong>Case report: </strong>A young male patient presented with acute chest pain following strenuous exertion. Initial outpatient evaluation, including complete blood count (CBC), liver function tests (LFTs), renal function tests (RFTs), cardiac enzymes, and chest X-ray (CXR), yielded nondiagnostic results, leading to his discharge with analgesics. Three days later, during a national holiday when outpatient clinics were closed, the patient returned to the emergency department (ED) with persistent chest pain. A meticulous review of the initial CXR by the emergency physician revealed mediastinal widening (measuring 8.5 cm) and an abnormal contour of the aorta. Subsequent emergency computed tomography angiography (CTA) confirmed the diagnosis of a Stanford type B aortic dissection.</p><p><strong>Conclusions: </strong>This case underscores two critical learning points: (1) the diagnostic pitfalls associated with atypical early presentations of aortic dissection, and (2) the often underappreciated value of meticulous interpretation of chest X-rays in the evaluation of acute chest pain, particularly when initial studies yield unremarkable results. The three-day diagnostic delay emphasizes the necessity of maintaining a high index of suspicion for aortic dissection, even in young patients lacking classic risk factors.</p>\",\"PeriodicalId\":13967,\"journal\":{\"name\":\"International Journal of Emergency Medicine\",\"volume\":\"18 1\",\"pages\":\"158\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382138/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s12245-025-00971-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12245-025-00971-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Delayed diagnosis of aortic dissection: the overlooked clues on chest X-ray.
Background: Acute aortic dissection (AD) is a life-threatening vascular emergency requiring immediate intervention, with mortality rates increasing by 1-2% per hour post-onset. The pathophysiology involves an intimal tear that permits blood to enter the medial layer, forming a false lumen that may expand and compromise branch vessels and end-organ perfusion. Current guidelines from the European Society of Cardiology (ESC), American College of Cardiology (ACC), and American Heart Association (AHA) highlight the necessity of risk stratification based on clinical features (e.g., tearing pain, pulse deficits), predisposing factors (e.g., hypertension), and D-dimer levels, followed by confirmatory imaging with transthoracic echocardiography (TTE) or computed tomography angiography (CTA). Despite advancements in imaging, chest radiography (CXR) remains underutilized; however, key findings-such as mediastinal widening (≥ 5 cm at the aortic knob), abnormal aortic contour, and displaced intimal calcifications-can offer critical diagnostic information.
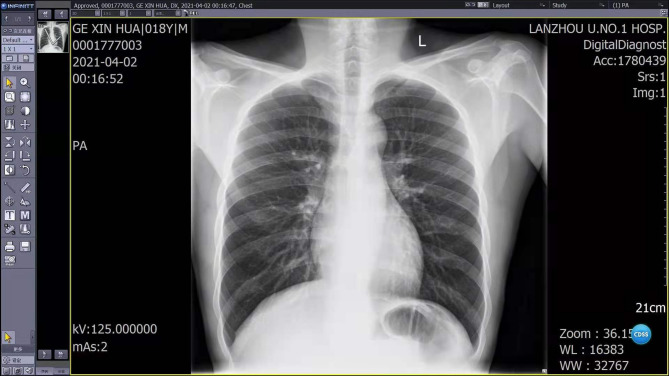
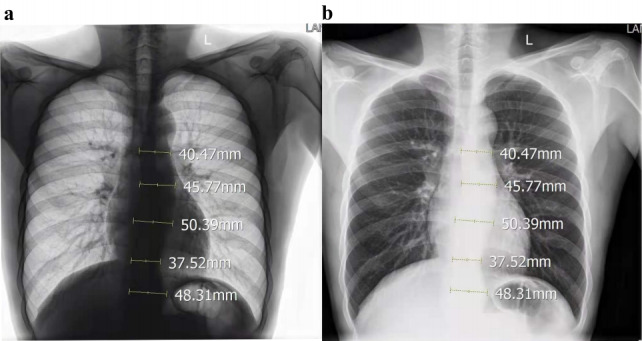
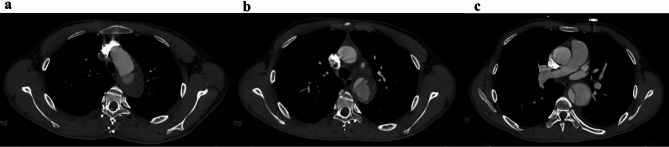
Case report: A young male patient presented with acute chest pain following strenuous exertion. Initial outpatient evaluation, including complete blood count (CBC), liver function tests (LFTs), renal function tests (RFTs), cardiac enzymes, and chest X-ray (CXR), yielded nondiagnostic results, leading to his discharge with analgesics. Three days later, during a national holiday when outpatient clinics were closed, the patient returned to the emergency department (ED) with persistent chest pain. A meticulous review of the initial CXR by the emergency physician revealed mediastinal widening (measuring 8.5 cm) and an abnormal contour of the aorta. Subsequent emergency computed tomography angiography (CTA) confirmed the diagnosis of a Stanford type B aortic dissection.
Conclusions: This case underscores two critical learning points: (1) the diagnostic pitfalls associated with atypical early presentations of aortic dissection, and (2) the often underappreciated value of meticulous interpretation of chest X-rays in the evaluation of acute chest pain, particularly when initial studies yield unremarkable results. The three-day diagnostic delay emphasizes the necessity of maintaining a high index of suspicion for aortic dissection, even in young patients lacking classic risk factors.
期刊介绍:
The aim of the journal is to bring to light the various clinical advancements and research developments attained over the world and thus help the specialty forge ahead. It is directed towards physicians and medical personnel undergoing training or working within the field of Emergency Medicine. Medical students who are interested in pursuing a career in Emergency Medicine will also benefit from the journal. This is particularly useful for trainees in countries where the specialty is still in its infancy. Disciplines covered will include interesting clinical cases, the latest evidence-based practice and research developments in Emergency medicine including emergency pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


