{"title":"左心室重构指数预测射血分数< 35的扩张型心肌病室性心动过速。","authors":"Xi Jia, Weipeng Yan, Xuan Ma, Zhixiang Dong, Jiaxin Wang, Shujuan Yang, Kankan Zhao, Zhuxin Wei, Yun Tang, Pengyu Zhou, Xingrui Chen, Yujie Liu, Xiuyu Chen, Shihua Zhao","doi":"10.1186/s13244-025-02059-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the left ventricular remodeling index (LVRI) for predicting ventricular tachyarrhythmia (VTA) in patients with dilated cardiomyopathy (DCM) with left ventricular ejection fraction (LVEF) < 35%.</p><p><strong>Materials and methods: </strong>In this retrospective single-center study, consecutive DCM patients with LVEF < 35% (n = 271) who underwent cardiac magnetic resonance (CMR) imaging were followed up. The study endpoint was VTA, including sudden cardiac death and major ventricular arrhythmias. The CMR-derived LVRI was defined as the cubic root of the LV end-diastolic volume divided by the maximal LV wall thickness. Competing risk regression analysis and Kaplan-Meier analysis were used to evaluate the association of LVRI with VTA.</p><p><strong>Results: </strong>Over 71-month median follow-up (interquartile range: 17-134 months), 35 (12.9%, mean age 46.7 years, 27 males) participants reached VTA events. The presence (62.9% vs. 60.2%, p = 0.761) and extent (6.9 ± 6.6 vs. 6.5 ± 8.3, p = 0.747) of late gadolinium enhancement (LGE) and LVEF (23.3 ± 6 vs. 21.9 ± 10.3, p = 0.197) were not significantly different between the patients with and without endpoint. Kaplan-Meier curve analysis showed that participants with LVRI ≥ 7.5 were more likely to experience VTA (p < 0.0001). In the multiple competing risk analysis, LVRI ≥ 7.5 (HR, 2.496; 95% CI: 1.213-5.138; p = 0.013) was observed as an independent predictor of VTA after adjusting for age, sex and left bundle branch block.</p><p><strong>Conclusions: </strong>For nonischemic DCM patients with LVEF < 35%, LVRI ≥ 7.5 was associated with lethal VTA events and provided incremental value over conventional CMR parameters.</p><p><strong>Critical relevance statement: </strong>The left ventricular remodeling index (LVRI) was independently associated with ventricular tachyarrhythmias in dilated cardiomyopathy patients with LVEF < 35%, and warrants future multicenter validation to assess incremental value over established predictors for implantable cardioverter-defibrillator decision-making.</p><p><strong>Key points: </strong>Left ventricular ejection fraction did not exhibit significant prognostic value for end-stage dilated cardiomyopathy patients. Cardiac MRI (CMR)-assessed left ventricular remodeling index (LVRI) ≥ 7.5 was an independent predictor of ventricular tachyarrhythmia. LVRI provided incremental prognostic value over conventional CMR parameters.</p>","PeriodicalId":13639,"journal":{"name":"Insights into Imaging","volume":"16 1","pages":"188"},"PeriodicalIF":4.5000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397014/pdf/","citationCount":"0","resultStr":"{\"title\":\"Left ventricular remodeling index to predict ventricular tachyarrhythmia in dilated cardiomyopathy with ejection fraction < 35.\",\"authors\":\"Xi Jia, Weipeng Yan, Xuan Ma, Zhixiang Dong, Jiaxin Wang, Shujuan Yang, Kankan Zhao, Zhuxin Wei, Yun Tang, Pengyu Zhou, Xingrui Chen, Yujie Liu, Xiuyu Chen, Shihua Zhao\",\"doi\":\"10.1186/s13244-025-02059-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess the left ventricular remodeling index (LVRI) for predicting ventricular tachyarrhythmia (VTA) in patients with dilated cardiomyopathy (DCM) with left ventricular ejection fraction (LVEF) < 35%.</p><p><strong>Materials and methods: </strong>In this retrospective single-center study, consecutive DCM patients with LVEF < 35% (n = 271) who underwent cardiac magnetic resonance (CMR) imaging were followed up. The study endpoint was VTA, including sudden cardiac death and major ventricular arrhythmias. The CMR-derived LVRI was defined as the cubic root of the LV end-diastolic volume divided by the maximal LV wall thickness. Competing risk regression analysis and Kaplan-Meier analysis were used to evaluate the association of LVRI with VTA.</p><p><strong>Results: </strong>Over 71-month median follow-up (interquartile range: 17-134 months), 35 (12.9%, mean age 46.7 years, 27 males) participants reached VTA events. The presence (62.9% vs. 60.2%, p = 0.761) and extent (6.9 ± 6.6 vs. 6.5 ± 8.3, p = 0.747) of late gadolinium enhancement (LGE) and LVEF (23.3 ± 6 vs. 21.9 ± 10.3, p = 0.197) were not significantly different between the patients with and without endpoint. Kaplan-Meier curve analysis showed that participants with LVRI ≥ 7.5 were more likely to experience VTA (p < 0.0001). In the multiple competing risk analysis, LVRI ≥ 7.5 (HR, 2.496; 95% CI: 1.213-5.138; p = 0.013) was observed as an independent predictor of VTA after adjusting for age, sex and left bundle branch block.</p><p><strong>Conclusions: </strong>For nonischemic DCM patients with LVEF < 35%, LVRI ≥ 7.5 was associated with lethal VTA events and provided incremental value over conventional CMR parameters.</p><p><strong>Critical relevance statement: </strong>The left ventricular remodeling index (LVRI) was independently associated with ventricular tachyarrhythmias in dilated cardiomyopathy patients with LVEF < 35%, and warrants future multicenter validation to assess incremental value over established predictors for implantable cardioverter-defibrillator decision-making.</p><p><strong>Key points: </strong>Left ventricular ejection fraction did not exhibit significant prognostic value for end-stage dilated cardiomyopathy patients. Cardiac MRI (CMR)-assessed left ventricular remodeling index (LVRI) ≥ 7.5 was an independent predictor of ventricular tachyarrhythmia. LVRI provided incremental prognostic value over conventional CMR parameters.</p>\",\"PeriodicalId\":13639,\"journal\":{\"name\":\"Insights into Imaging\",\"volume\":\"16 1\",\"pages\":\"188\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397014/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Insights into Imaging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13244-025-02059-6\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Insights into Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13244-025-02059-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Left ventricular remodeling index to predict ventricular tachyarrhythmia in dilated cardiomyopathy with ejection fraction < 35.
Objectives: To assess the left ventricular remodeling index (LVRI) for predicting ventricular tachyarrhythmia (VTA) in patients with dilated cardiomyopathy (DCM) with left ventricular ejection fraction (LVEF) < 35%.
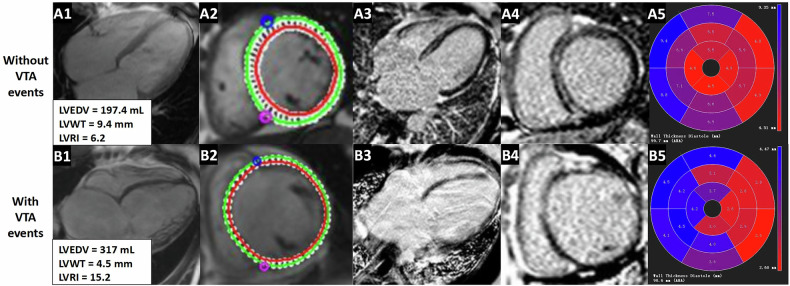
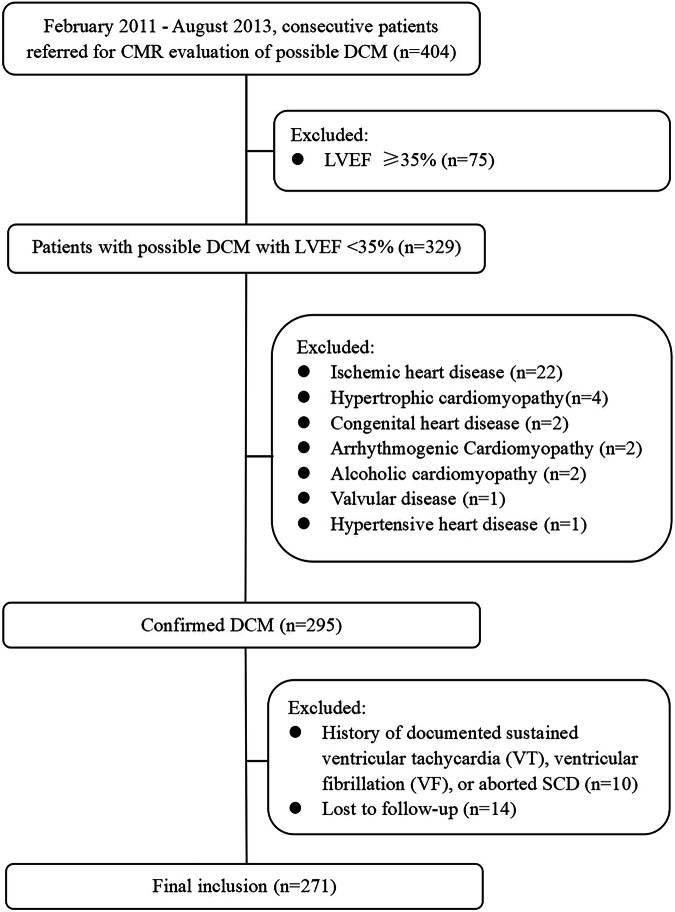
Materials and methods: In this retrospective single-center study, consecutive DCM patients with LVEF < 35% (n = 271) who underwent cardiac magnetic resonance (CMR) imaging were followed up. The study endpoint was VTA, including sudden cardiac death and major ventricular arrhythmias. The CMR-derived LVRI was defined as the cubic root of the LV end-diastolic volume divided by the maximal LV wall thickness. Competing risk regression analysis and Kaplan-Meier analysis were used to evaluate the association of LVRI with VTA.
Results: Over 71-month median follow-up (interquartile range: 17-134 months), 35 (12.9%, mean age 46.7 years, 27 males) participants reached VTA events. The presence (62.9% vs. 60.2%, p = 0.761) and extent (6.9 ± 6.6 vs. 6.5 ± 8.3, p = 0.747) of late gadolinium enhancement (LGE) and LVEF (23.3 ± 6 vs. 21.9 ± 10.3, p = 0.197) were not significantly different between the patients with and without endpoint. Kaplan-Meier curve analysis showed that participants with LVRI ≥ 7.5 were more likely to experience VTA (p < 0.0001). In the multiple competing risk analysis, LVRI ≥ 7.5 (HR, 2.496; 95% CI: 1.213-5.138; p = 0.013) was observed as an independent predictor of VTA after adjusting for age, sex and left bundle branch block.
Conclusions: For nonischemic DCM patients with LVEF < 35%, LVRI ≥ 7.5 was associated with lethal VTA events and provided incremental value over conventional CMR parameters.
Critical relevance statement: The left ventricular remodeling index (LVRI) was independently associated with ventricular tachyarrhythmias in dilated cardiomyopathy patients with LVEF < 35%, and warrants future multicenter validation to assess incremental value over established predictors for implantable cardioverter-defibrillator decision-making.
Key points: Left ventricular ejection fraction did not exhibit significant prognostic value for end-stage dilated cardiomyopathy patients. Cardiac MRI (CMR)-assessed left ventricular remodeling index (LVRI) ≥ 7.5 was an independent predictor of ventricular tachyarrhythmia. LVRI provided incremental prognostic value over conventional CMR parameters.
期刊介绍:
Insights into Imaging (I³) is a peer-reviewed open access journal published under the brand SpringerOpen. All content published in the journal is freely available online to anyone, anywhere!
I³ continuously updates scientific knowledge and progress in best-practice standards in radiology through the publication of original articles and state-of-the-art reviews and opinions, along with recommendations and statements from the leading radiological societies in Europe.
Founded by the European Society of Radiology (ESR), I³ creates a platform for educational material, guidelines and recommendations, and a forum for topics of controversy.
A balanced combination of review articles, original papers, short communications from European radiological congresses and information on society matters makes I³ an indispensable source for current information in this field.
I³ is owned by the ESR, however authors retain copyright to their article according to the Creative Commons Attribution License (see Copyright and License Agreement). All articles can be read, redistributed and reused for free, as long as the author of the original work is cited properly.
The open access fees (article-processing charges) for this journal are kindly sponsored by ESR for all Members.
The journal went open access in 2012, which means that all articles published since then are freely available online.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


