Jarieke C Hoogendoorn, Laurens P Bosman, Jeroen F van der Heijden, Arthur A Wilde, Maarten P van den Berg, Sing-Chien Yap, J Peter van Tintelen, Dennis Dooijes, Anneline S J M Te Riele, Katja Zeppenfeld
{"title":"室性心动过速患者的不同潜在病因符合致心律失常右室心肌病工作组标准:基于12导联心电图的初步怀疑。","authors":"Jarieke C Hoogendoorn, Laurens P Bosman, Jeroen F van der Heijden, Arthur A Wilde, Maarten P van den Berg, Sing-Chien Yap, J Peter van Tintelen, Dennis Dooijes, Anneline S J M Te Riele, Katja Zeppenfeld","doi":"10.1093/europace/euaf136","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The task force criteria (TFC) for arrhythmogenic right ventricular cardiomyopathy (ARVC) are highly sensitive but lack specificity. Atypical RV involvement (aRVi) may indicate different underlying aetiologies and prognosis, requiring specific therapeutic interventions. We aimed to evaluate the role of the baseline 12-lead ECG for initial suspicion of aRVi.</p><p><strong>Methods: </strong>From the Netherlands Heart Institute Arrhythmogenic Cardiomyopathy (NHI-ACM) registry, patients were selected who (i) fulfilled TFC for definite ARVC, (ii) presented with sustained ventricular tachycardia (VT), and (iii) underwent genetic testing. The first available ECG after VT was evaluated. PR prolongation ≥220 ms and/or a surface area of the maximum R'-wave in V1-V3 of ≥1.65 mm2 was defined as an aRVi-ECG. Patients with an ARVC-related pathogenic/likely pathogenic variant (P/LP+) were classified as 'ARVC'. Data of P/LP- were reviewed by an expert panel and classified as either 'ARVC' or 'different aetiology' based on consensus.</p><p><strong>Results: </strong>A total of 159 patients were included (122 P/LP+ and 37 P/LP- patients). Nineteen patients had an aRVi-ECG [11 (9%) P/LP+ vs. 8 (22%) P/LP-, P = 0.038]. Of the P/LP- patients, 17 (46%) were classified as 'different aetiology' (e.g. myocarditis, ischaemia, sarcoidosis), including all 8 patients with an aRVi-ECG. Among the P/LP+ patients with an aRVi-ECG, 46% carried the p.Arg14del phospholamban pathogenic variant, and 64% died compared to 15 and 19% of P/LP+ patients without an aRVi-ECG, respectively (both P < 0.01).</p><p><strong>Conclusion: </strong>In P/LP- patients presenting with VT and fulfilling TFC, an aRVi-ECG should raise suspicion for a different underlying aetiology. In P/LP+ patients, an aRVi-ECG may identify those with poor outcome.</p>","PeriodicalId":11981,"journal":{"name":"Europace","volume":"27 8","pages":""},"PeriodicalIF":7.4000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12365759/pdf/","citationCount":"0","resultStr":"{\"title\":\"Different underlying aetiologies in patients presenting with ventricular tachycardia fulfilling task force criteria for arrhythmogenic right ventricular cardiomyopathy: initial suspicion based on the 12-lead electrocardiogram.\",\"authors\":\"Jarieke C Hoogendoorn, Laurens P Bosman, Jeroen F van der Heijden, Arthur A Wilde, Maarten P van den Berg, Sing-Chien Yap, J Peter van Tintelen, Dennis Dooijes, Anneline S J M Te Riele, Katja Zeppenfeld\",\"doi\":\"10.1093/europace/euaf136\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The task force criteria (TFC) for arrhythmogenic right ventricular cardiomyopathy (ARVC) are highly sensitive but lack specificity. Atypical RV involvement (aRVi) may indicate different underlying aetiologies and prognosis, requiring specific therapeutic interventions. We aimed to evaluate the role of the baseline 12-lead ECG for initial suspicion of aRVi.</p><p><strong>Methods: </strong>From the Netherlands Heart Institute Arrhythmogenic Cardiomyopathy (NHI-ACM) registry, patients were selected who (i) fulfilled TFC for definite ARVC, (ii) presented with sustained ventricular tachycardia (VT), and (iii) underwent genetic testing. The first available ECG after VT was evaluated. PR prolongation ≥220 ms and/or a surface area of the maximum R'-wave in V1-V3 of ≥1.65 mm2 was defined as an aRVi-ECG. Patients with an ARVC-related pathogenic/likely pathogenic variant (P/LP+) were classified as 'ARVC'. Data of P/LP- were reviewed by an expert panel and classified as either 'ARVC' or 'different aetiology' based on consensus.</p><p><strong>Results: </strong>A total of 159 patients were included (122 P/LP+ and 37 P/LP- patients). Nineteen patients had an aRVi-ECG [11 (9%) P/LP+ vs. 8 (22%) P/LP-, P = 0.038]. Of the P/LP- patients, 17 (46%) were classified as 'different aetiology' (e.g. myocarditis, ischaemia, sarcoidosis), including all 8 patients with an aRVi-ECG. Among the P/LP+ patients with an aRVi-ECG, 46% carried the p.Arg14del phospholamban pathogenic variant, and 64% died compared to 15 and 19% of P/LP+ patients without an aRVi-ECG, respectively (both P < 0.01).</p><p><strong>Conclusion: </strong>In P/LP- patients presenting with VT and fulfilling TFC, an aRVi-ECG should raise suspicion for a different underlying aetiology. In P/LP+ patients, an aRVi-ECG may identify those with poor outcome.</p>\",\"PeriodicalId\":11981,\"journal\":{\"name\":\"Europace\",\"volume\":\"27 8\",\"pages\":\"\"},\"PeriodicalIF\":7.4000,\"publicationDate\":\"2025-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12365759/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Europace\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/europace/euaf136\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Europace","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/europace/euaf136","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:致心律失常性右室心肌病(ARVC)的工作小组标准(TFC)高度敏感,但缺乏特异性。非典型RV受累(aRVi)可能表明不同的潜在病因和预后,需要特定的治疗干预。我们的目的是评估基线12导联心电图对aRVi初步怀疑的作用。方法:从荷兰心脏研究所致心律失常心肌病(NHI-ACM)登记处选择(i)满足TFC的明确ARVC患者,(ii)持续室性心动过速(VT), (iii)接受基因检测的患者。评估室性心动过速后的第一个可用心电图。PR延长≥220 ms和/或V1-V3最大R′波表面积≥1.65 mm2定义为aRVi-ECG。具有ARVC相关致病/可能致病变异(P/LP+)的患者被归类为“ARVC”。专家小组审查了P/LP-的数据,并根据共识将其分类为“ARVC”或“不同病因”。结果:共纳入159例患者(P/LP+患者122例,P/LP-患者37例)。19例患者有aRVi-ECG[11例(9%)P/LP+ vs. 8例(22%)P/LP-, P = 0.038]。在P/LP-患者中,17例(46%)被分类为“不同病因”(如心肌炎、缺血、结节病),包括所有8例aRVi-ECG患者。在伴有aRVi-ECG的P/LP+患者中,46%的患者携带p.a g14del磷蛋白致病变异,64%的患者死亡,而无aRVi-ECG的P/LP+患者的死亡率分别为15%和19% (P < 0.01)。结论:在出现VT和TFC的P/LP患者中,aRVi-ECG应该引起对不同潜在病因的怀疑。在P/LP+患者中,aRVi-ECG可以识别出预后不良的患者。
Different underlying aetiologies in patients presenting with ventricular tachycardia fulfilling task force criteria for arrhythmogenic right ventricular cardiomyopathy: initial suspicion based on the 12-lead electrocardiogram.
Aims: The task force criteria (TFC) for arrhythmogenic right ventricular cardiomyopathy (ARVC) are highly sensitive but lack specificity. Atypical RV involvement (aRVi) may indicate different underlying aetiologies and prognosis, requiring specific therapeutic interventions. We aimed to evaluate the role of the baseline 12-lead ECG for initial suspicion of aRVi.
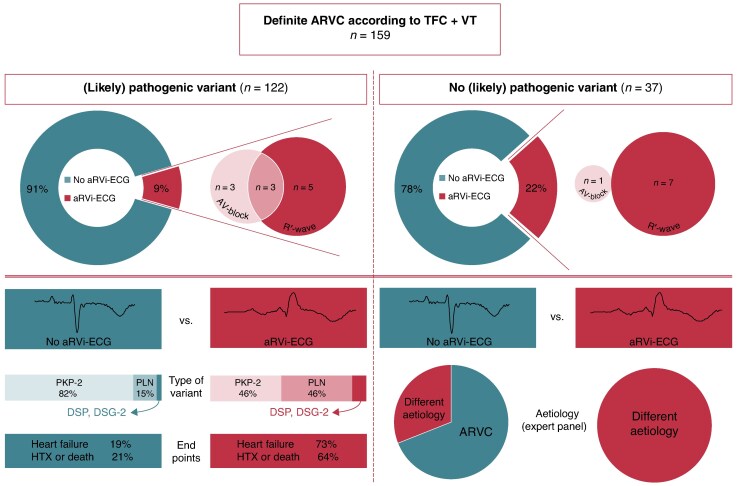
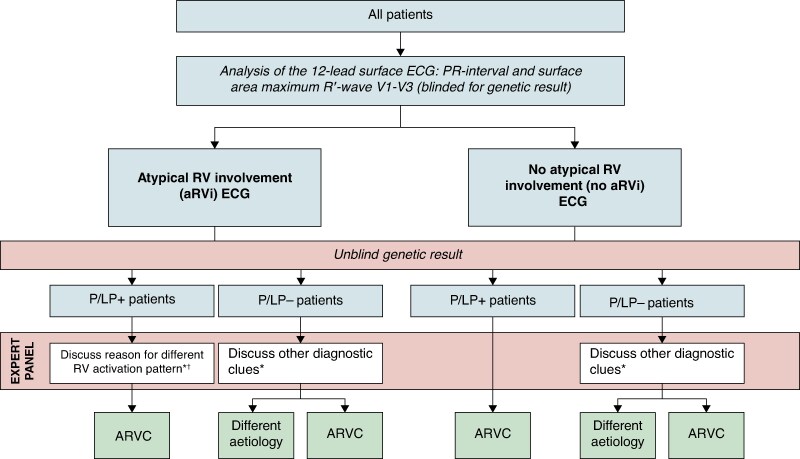
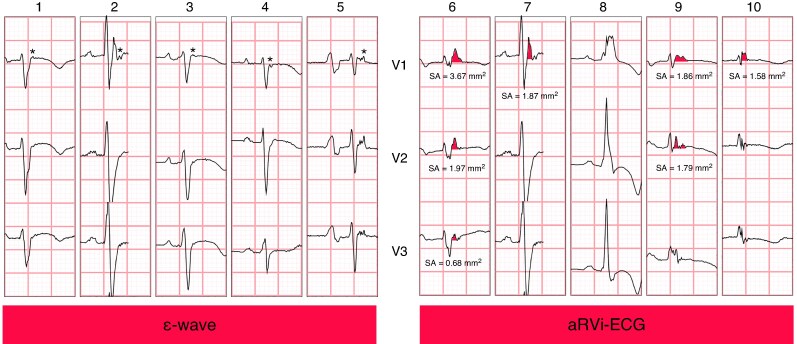
Methods: From the Netherlands Heart Institute Arrhythmogenic Cardiomyopathy (NHI-ACM) registry, patients were selected who (i) fulfilled TFC for definite ARVC, (ii) presented with sustained ventricular tachycardia (VT), and (iii) underwent genetic testing. The first available ECG after VT was evaluated. PR prolongation ≥220 ms and/or a surface area of the maximum R'-wave in V1-V3 of ≥1.65 mm2 was defined as an aRVi-ECG. Patients with an ARVC-related pathogenic/likely pathogenic variant (P/LP+) were classified as 'ARVC'. Data of P/LP- were reviewed by an expert panel and classified as either 'ARVC' or 'different aetiology' based on consensus.
Results: A total of 159 patients were included (122 P/LP+ and 37 P/LP- patients). Nineteen patients had an aRVi-ECG [11 (9%) P/LP+ vs. 8 (22%) P/LP-, P = 0.038]. Of the P/LP- patients, 17 (46%) were classified as 'different aetiology' (e.g. myocarditis, ischaemia, sarcoidosis), including all 8 patients with an aRVi-ECG. Among the P/LP+ patients with an aRVi-ECG, 46% carried the p.Arg14del phospholamban pathogenic variant, and 64% died compared to 15 and 19% of P/LP+ patients without an aRVi-ECG, respectively (both P < 0.01).
Conclusion: In P/LP- patients presenting with VT and fulfilling TFC, an aRVi-ECG should raise suspicion for a different underlying aetiology. In P/LP+ patients, an aRVi-ECG may identify those with poor outcome.
期刊介绍:
EP - Europace - European Journal of Pacing, Arrhythmias and Cardiac Electrophysiology of the European Heart Rhythm Association of the European Society of Cardiology. The journal aims to provide an avenue of communication of top quality European and international original scientific work and reviews in the fields of Arrhythmias, Pacing and Cellular Electrophysiology. The Journal offers the reader a collection of contemporary original peer-reviewed papers, invited papers and editorial comments together with book reviews and correspondence.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


