Fabio Rotondo, Sofia Siena, Maria Rosa Pastore, Pasquale Pio Maccarone, Morena Luce Mansueto, Irene Rutigliano
{"title":"双侧输尿管结石合并肾后急性肾损伤:一罕见的糖尿病酮症酸中毒患儿并发症。","authors":"Fabio Rotondo, Sofia Siena, Maria Rosa Pastore, Pasquale Pio Maccarone, Morena Luce Mansueto, Irene Rutigliano","doi":"10.1155/crpe/2711257","DOIUrl":null,"url":null,"abstract":"<p><p>Diabetic ketoacidosis (DKA) is a common initial presentation of type 1 diabetes mellitus (T1DM) in children occurring in up to 40% of cases. DKA can also be associated with severe complications, including nephrolithiasis. We present the case of a 12 years and 8-month-old boy who developed acute kidney injury (AKI) secondary to bilateral urinary lithiasis during the onset of T1DM with DKA. After conventional treatment for DKA, laboratory tests showed increased creatinine and azotemia. 24 hours later, he developed lumbar pain and anuria. Plain radiography, ultrasonography, and computed tomography (CT) revealed bilateral renal calculi and pelvic dilation. An urgent bilateral ascending pyelography with stent placement was performed. Right ureteral stenting was successful, but left stenting failed due to an intramural ureteral anatomical variant; thus, a nephrostomy was performed. Diuresis resumed immediately, and renal function normalized over the following days without permanent impairment. To our knowledge, this is the first reported case of bilateral lithiasis with ureteral stenosis in a pediatric patient with DKA. In patients with severe DKA, we recommend routine monitoring of kidney function with a low threshold for CT imaging whenever there is an unexpected rise in creatinine, oliguria/anuria, or lumbar pain. Early multidisciplinary intervention can promptly relieve postrenal obstruction, prevent permanent renal damage, and improve outcomes.</p>","PeriodicalId":9623,"journal":{"name":"Case Reports in Pediatrics","volume":"2025 ","pages":"2711257"},"PeriodicalIF":0.5000,"publicationDate":"2025-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12373468/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bilateral Ureteral Lithiasis and Postrenal Acute Kidney Injury: A Rare Complication of Diabetic Ketoacidosis in a Child.\",\"authors\":\"Fabio Rotondo, Sofia Siena, Maria Rosa Pastore, Pasquale Pio Maccarone, Morena Luce Mansueto, Irene Rutigliano\",\"doi\":\"10.1155/crpe/2711257\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Diabetic ketoacidosis (DKA) is a common initial presentation of type 1 diabetes mellitus (T1DM) in children occurring in up to 40% of cases. DKA can also be associated with severe complications, including nephrolithiasis. We present the case of a 12 years and 8-month-old boy who developed acute kidney injury (AKI) secondary to bilateral urinary lithiasis during the onset of T1DM with DKA. After conventional treatment for DKA, laboratory tests showed increased creatinine and azotemia. 24 hours later, he developed lumbar pain and anuria. Plain radiography, ultrasonography, and computed tomography (CT) revealed bilateral renal calculi and pelvic dilation. An urgent bilateral ascending pyelography with stent placement was performed. Right ureteral stenting was successful, but left stenting failed due to an intramural ureteral anatomical variant; thus, a nephrostomy was performed. Diuresis resumed immediately, and renal function normalized over the following days without permanent impairment. To our knowledge, this is the first reported case of bilateral lithiasis with ureteral stenosis in a pediatric patient with DKA. In patients with severe DKA, we recommend routine monitoring of kidney function with a low threshold for CT imaging whenever there is an unexpected rise in creatinine, oliguria/anuria, or lumbar pain. Early multidisciplinary intervention can promptly relieve postrenal obstruction, prevent permanent renal damage, and improve outcomes.</p>\",\"PeriodicalId\":9623,\"journal\":{\"name\":\"Case Reports in Pediatrics\",\"volume\":\"2025 \",\"pages\":\"2711257\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2025-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12373468/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Pediatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crpe/2711257\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crpe/2711257","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
Bilateral Ureteral Lithiasis and Postrenal Acute Kidney Injury: A Rare Complication of Diabetic Ketoacidosis in a Child.
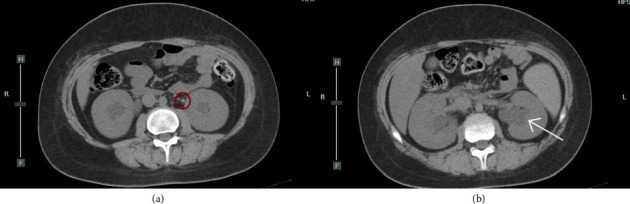
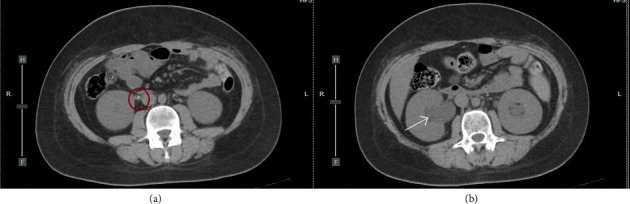
Diabetic ketoacidosis (DKA) is a common initial presentation of type 1 diabetes mellitus (T1DM) in children occurring in up to 40% of cases. DKA can also be associated with severe complications, including nephrolithiasis. We present the case of a 12 years and 8-month-old boy who developed acute kidney injury (AKI) secondary to bilateral urinary lithiasis during the onset of T1DM with DKA. After conventional treatment for DKA, laboratory tests showed increased creatinine and azotemia. 24 hours later, he developed lumbar pain and anuria. Plain radiography, ultrasonography, and computed tomography (CT) revealed bilateral renal calculi and pelvic dilation. An urgent bilateral ascending pyelography with stent placement was performed. Right ureteral stenting was successful, but left stenting failed due to an intramural ureteral anatomical variant; thus, a nephrostomy was performed. Diuresis resumed immediately, and renal function normalized over the following days without permanent impairment. To our knowledge, this is the first reported case of bilateral lithiasis with ureteral stenosis in a pediatric patient with DKA. In patients with severe DKA, we recommend routine monitoring of kidney function with a low threshold for CT imaging whenever there is an unexpected rise in creatinine, oliguria/anuria, or lumbar pain. Early multidisciplinary intervention can promptly relieve postrenal obstruction, prevent permanent renal damage, and improve outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


