{"title":"与通气参数和肺部疾病相关的心律失常事件:来自两项前瞻性队列研究的证据","authors":"Yun-Jiu Cheng, Li-Ping Qu, Yi-Jian Liao, Si-Long Lu, Mei-Ping Lin, Qian He, Jin-Bo Fu, Jun-Chi Li, Wen-Juan Duan, Li-Juan Liu","doi":"10.1186/s12916-025-04345-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emerging epidemiological evidence implicates pulmonary dysfunction in cardiovascular pathogenesis, yet its arrhythmogenic potential remains poorly defined.</p><p><strong>Objectives: </strong>We aimed to assess the link between ventilatory parameters, pulmonary disease phenotypes and risk of incident arrhythmias across diverse populations.</p><p><strong>Methods: </strong>We analyzed data from 17,684 adults in two prospective cohort studies-the Atherosclerosis Risk in Communities (ARIC; n = 12,929) and Cardiovascular Health Study (CHS; n = 4,755). Adjudicated arrhythmia diagnoses (atrial fibrillation/flutter [AF/AFL], ventricular arrhythmias [VAs], high-grade atrioventricular [AV] block, and premature atrial/ventricular complexes [PAC/PVC]) were identified via hospitalization records and mortality data. Multivariable-adjusted Cox proportional hazards models quantified associations between forced expiratory volume in 1 s (FEV1%) predicted and forced vital capacity (FVC%) predicted quartiles with arrhythmia risk, adjusting for traditional cardiovascular risk factors.</p><p><strong>Results: </strong>Over a median follow-up of 12.6 years, impaired FEV1% and FVC% corresponded to a graded increase in arrhythmia risk. Compared to the highest quartile, the lowest FEV1% predicted quartile had elevated hazards for any arrhythmias (HR 1.32, 95% CI 1.23-1.42), AF/AFL (HR 1.68, 1.52-1.85), VAs (HR 1.55, 1.29-1.86), high-grade AV block (HR 1.37, 1.08-1.73), and PAC/PVC (HR 1.42, 1.20-1.69). Similar trends were observed for FVC% predicted quartiles. These associations remained consistent in never-smoking individuals and across cohorts. Obstructive spirometry pattern was associated with the strongest arrhythmia risk, while restrictive ventilatory patterns showed relatively lower risk elevations. No association was observed with sick sinus syndrome.</p><p><strong>Conclusions: </strong>Reduced pulmonary function suggested independent associations with incident arrhythmias across supraventricular, ventricular, and conduction system pathologies in two historical cohorts. These findings suggest that spirometric indices could potentially represent novel independent indicators for arrhythmia development worthy of further validation in contemporary settings,, with associations distinct from conventional cardiometabolic risk factors.</p>","PeriodicalId":9188,"journal":{"name":"BMC Medicine","volume":"23 1","pages":"493"},"PeriodicalIF":8.3000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374318/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incident arrhythmias in relation to ventilatory parameters and pulmonary disease: evidence from two prospective cohort studies.\",\"authors\":\"Yun-Jiu Cheng, Li-Ping Qu, Yi-Jian Liao, Si-Long Lu, Mei-Ping Lin, Qian He, Jin-Bo Fu, Jun-Chi Li, Wen-Juan Duan, Li-Juan Liu\",\"doi\":\"10.1186/s12916-025-04345-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Emerging epidemiological evidence implicates pulmonary dysfunction in cardiovascular pathogenesis, yet its arrhythmogenic potential remains poorly defined.</p><p><strong>Objectives: </strong>We aimed to assess the link between ventilatory parameters, pulmonary disease phenotypes and risk of incident arrhythmias across diverse populations.</p><p><strong>Methods: </strong>We analyzed data from 17,684 adults in two prospective cohort studies-the Atherosclerosis Risk in Communities (ARIC; n = 12,929) and Cardiovascular Health Study (CHS; n = 4,755). Adjudicated arrhythmia diagnoses (atrial fibrillation/flutter [AF/AFL], ventricular arrhythmias [VAs], high-grade atrioventricular [AV] block, and premature atrial/ventricular complexes [PAC/PVC]) were identified via hospitalization records and mortality data. Multivariable-adjusted Cox proportional hazards models quantified associations between forced expiratory volume in 1 s (FEV1%) predicted and forced vital capacity (FVC%) predicted quartiles with arrhythmia risk, adjusting for traditional cardiovascular risk factors.</p><p><strong>Results: </strong>Over a median follow-up of 12.6 years, impaired FEV1% and FVC% corresponded to a graded increase in arrhythmia risk. Compared to the highest quartile, the lowest FEV1% predicted quartile had elevated hazards for any arrhythmias (HR 1.32, 95% CI 1.23-1.42), AF/AFL (HR 1.68, 1.52-1.85), VAs (HR 1.55, 1.29-1.86), high-grade AV block (HR 1.37, 1.08-1.73), and PAC/PVC (HR 1.42, 1.20-1.69). Similar trends were observed for FVC% predicted quartiles. These associations remained consistent in never-smoking individuals and across cohorts. Obstructive spirometry pattern was associated with the strongest arrhythmia risk, while restrictive ventilatory patterns showed relatively lower risk elevations. No association was observed with sick sinus syndrome.</p><p><strong>Conclusions: </strong>Reduced pulmonary function suggested independent associations with incident arrhythmias across supraventricular, ventricular, and conduction system pathologies in two historical cohorts. These findings suggest that spirometric indices could potentially represent novel independent indicators for arrhythmia development worthy of further validation in contemporary settings,, with associations distinct from conventional cardiometabolic risk factors.</p>\",\"PeriodicalId\":9188,\"journal\":{\"name\":\"BMC Medicine\",\"volume\":\"23 1\",\"pages\":\"493\"},\"PeriodicalIF\":8.3000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374318/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12916-025-04345-y\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12916-025-04345-y","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:新出现的流行病学证据表明肺功能障碍与心血管发病机制有关,但其致心律失常的潜力仍不明确。目的:我们旨在评估不同人群中通气参数、肺部疾病表型和发生心律失常风险之间的联系。方法:我们分析了来自社区动脉粥样硬化风险(ARIC, n = 12,929)和心血管健康研究(CHS, n = 4,755)两项前瞻性队列研究中的17,684名成年人的数据。通过住院记录和死亡率数据确定已确诊的心律失常诊断(心房颤动/扑动[AF/AFL]、室性心律失常[VAs]、高级别房室传导阻滞和过早房室复合[PAC/PVC])。多变量调整的Cox比例风险模型量化了1秒内用力呼气量(FEV1%)预测与用力肺活量(FVC%)预测与心律失常风险的四分位数之间的关联,并对传统的心血管危险因素进行了调整。结果:在中位12.6年的随访中,FEV1%和FVC%的损伤对应于心律失常风险的分级增加。与最高四分位数相比,最低FEV1%预测四分位数的任何心律失常(HR 1.32, 95% CI 1.23-1.42)、AF/AFL (HR 1.68, 1.52-1.85)、VAs (HR 1.55, 1.29-1.86)、高级别房室传导阻滞(HR 1.37, 1.08-1.73)和PAC/PVC (HR 1.42, 1.20-1.69)的风险均升高。FVC%预测四分位数也观察到类似的趋势。这些关联在从不吸烟的个体和人群中保持一致。阻塞性肺活量测定模式与最强心律失常风险相关,而限制性通气模式的风险升高相对较低。与病窦综合征无关联。结论:在两个历史队列中,肺功能降低提示与室上、室和传导系统病理中发生的心律失常有独立关联。这些发现表明,肺活量测定指标可能代表心律失常发展的新的独立指标,值得在当代环境中进一步验证,与传统的心脏代谢危险因素有不同的关联。
Incident arrhythmias in relation to ventilatory parameters and pulmonary disease: evidence from two prospective cohort studies.
Background: Emerging epidemiological evidence implicates pulmonary dysfunction in cardiovascular pathogenesis, yet its arrhythmogenic potential remains poorly defined.
Objectives: We aimed to assess the link between ventilatory parameters, pulmonary disease phenotypes and risk of incident arrhythmias across diverse populations.
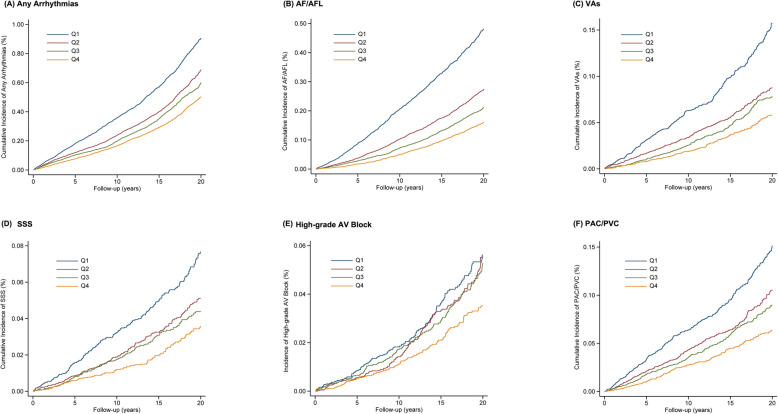
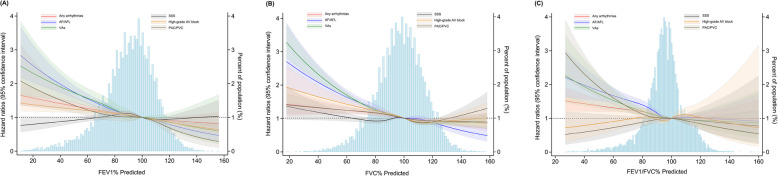
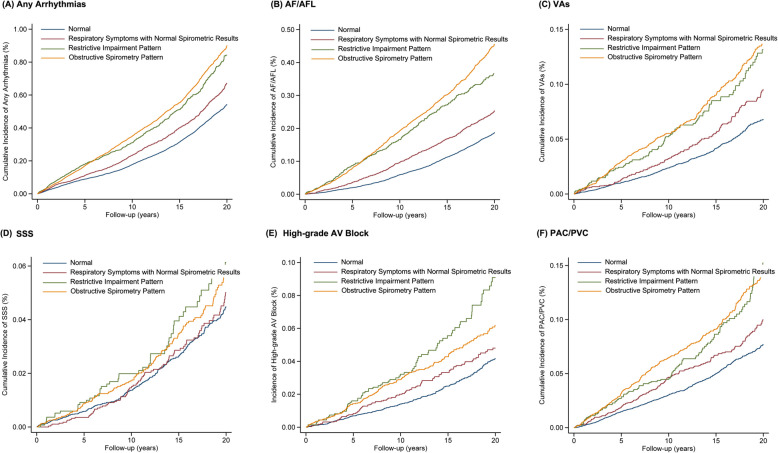
Methods: We analyzed data from 17,684 adults in two prospective cohort studies-the Atherosclerosis Risk in Communities (ARIC; n = 12,929) and Cardiovascular Health Study (CHS; n = 4,755). Adjudicated arrhythmia diagnoses (atrial fibrillation/flutter [AF/AFL], ventricular arrhythmias [VAs], high-grade atrioventricular [AV] block, and premature atrial/ventricular complexes [PAC/PVC]) were identified via hospitalization records and mortality data. Multivariable-adjusted Cox proportional hazards models quantified associations between forced expiratory volume in 1 s (FEV1%) predicted and forced vital capacity (FVC%) predicted quartiles with arrhythmia risk, adjusting for traditional cardiovascular risk factors.
Results: Over a median follow-up of 12.6 years, impaired FEV1% and FVC% corresponded to a graded increase in arrhythmia risk. Compared to the highest quartile, the lowest FEV1% predicted quartile had elevated hazards for any arrhythmias (HR 1.32, 95% CI 1.23-1.42), AF/AFL (HR 1.68, 1.52-1.85), VAs (HR 1.55, 1.29-1.86), high-grade AV block (HR 1.37, 1.08-1.73), and PAC/PVC (HR 1.42, 1.20-1.69). Similar trends were observed for FVC% predicted quartiles. These associations remained consistent in never-smoking individuals and across cohorts. Obstructive spirometry pattern was associated with the strongest arrhythmia risk, while restrictive ventilatory patterns showed relatively lower risk elevations. No association was observed with sick sinus syndrome.
Conclusions: Reduced pulmonary function suggested independent associations with incident arrhythmias across supraventricular, ventricular, and conduction system pathologies in two historical cohorts. These findings suggest that spirometric indices could potentially represent novel independent indicators for arrhythmia development worthy of further validation in contemporary settings,, with associations distinct from conventional cardiometabolic risk factors.
期刊介绍:
BMC Medicine is an open access, transparent peer-reviewed general medical journal. It is the flagship journal of the BMC series and publishes outstanding and influential research in various areas including clinical practice, translational medicine, medical and health advances, public health, global health, policy, and general topics of interest to the biomedical and sociomedical professional communities. In addition to research articles, the journal also publishes stimulating debates, reviews, unique forum articles, and concise tutorials. All articles published in BMC Medicine are included in various databases such as Biological Abstracts, BIOSIS, CAS, Citebase, Current contents, DOAJ, Embase, MEDLINE, PubMed, Science Citation Index Expanded, OAIster, SCImago, Scopus, SOCOLAR, and Zetoc.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


