Markus Schichtel, Stephen Barclay, Helena Papworth, Leila Mills, Ben Bowers
{"title":"以药剂师为主导的指导心力衰竭的药物治疗:对初级保健的影响分析","authors":"Markus Schichtel, Stephen Barclay, Helena Papworth, Leila Mills, Ben Bowers","doi":"10.1136/bmjoq-2025-003401","DOIUrl":null,"url":null,"abstract":"<p><p>Optimal guideline-directed medical therapy (GDMT) can reduce mortality, unplanned hospital admissions and improve quality of life for patients suffering from heart failure (HF). However, GDMT remains underused in primary care. Only a minority of patients on HF registers receive optimal GDMT in the UK. This suboptimal care is compounded by a mounting lack of GP capacity and the growing burden of HF.A multisite, quantitative impact analysis was undertaken to evaluate the optimisation of HF patients by a novel pharmacist-led GDMT model in UK primary care.We identified low-risk HF patients suitable for pharmacists' input, including a community validated risk stratification tool-the HF Event STrengthening Score. The primary outcome was to compare the proportion of patients on optimal HF GDMT at 6 months and 2 years with baseline. Secondary outcomes were direct personnel healthcare costs and GP workload. A subgroup analysis was modelled to estimate effect on mortality, hospitalisation and quality of life.A total of 237 patients were included. Pharmacist-led GDMT contributed to the increase of optimal GDMT from 17.7% at baseline to 76.5% at 6 months and 94.5% at 2 years follow-up. The novel approach reduced GPs' HF GDMT workload by 36.6% at 6 months and 42.1% at 2 years and healthcare costs by 18.4% at 6 months and 20.3% at 2 years. Patients with combined angiotensin receptor neprilysin inhibitor/sodium glucose co-transporter 2 inhibitor treatment indicated a reduction of 20.8% in cardiovascular mortality, a reduction of 34.8% in hospitalisations and a 5.31 Kansas City Cardiomyopathy Questionnaire Score for improved quality of life at 2 years.For low-risk HF patients, pharmacist-led optimisation achieved significantly higher GDMT rates, reduced personnel healthcare costs, reduced GPs' workload, contributed to reduced cardiovascular mortality, reduced hospitalisations and improved quality of life. In the context of current workload pressures, this approach should be considered for widespread implementation in general practice.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"14 3","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406906/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pharmacist-led guideline-directed medical therapy in heart failure: impact analysis in primary care.\",\"authors\":\"Markus Schichtel, Stephen Barclay, Helena Papworth, Leila Mills, Ben Bowers\",\"doi\":\"10.1136/bmjoq-2025-003401\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Optimal guideline-directed medical therapy (GDMT) can reduce mortality, unplanned hospital admissions and improve quality of life for patients suffering from heart failure (HF). However, GDMT remains underused in primary care. Only a minority of patients on HF registers receive optimal GDMT in the UK. This suboptimal care is compounded by a mounting lack of GP capacity and the growing burden of HF.A multisite, quantitative impact analysis was undertaken to evaluate the optimisation of HF patients by a novel pharmacist-led GDMT model in UK primary care.We identified low-risk HF patients suitable for pharmacists' input, including a community validated risk stratification tool-the HF Event STrengthening Score. The primary outcome was to compare the proportion of patients on optimal HF GDMT at 6 months and 2 years with baseline. Secondary outcomes were direct personnel healthcare costs and GP workload. A subgroup analysis was modelled to estimate effect on mortality, hospitalisation and quality of life.A total of 237 patients were included. Pharmacist-led GDMT contributed to the increase of optimal GDMT from 17.7% at baseline to 76.5% at 6 months and 94.5% at 2 years follow-up. The novel approach reduced GPs' HF GDMT workload by 36.6% at 6 months and 42.1% at 2 years and healthcare costs by 18.4% at 6 months and 20.3% at 2 years. Patients with combined angiotensin receptor neprilysin inhibitor/sodium glucose co-transporter 2 inhibitor treatment indicated a reduction of 20.8% in cardiovascular mortality, a reduction of 34.8% in hospitalisations and a 5.31 Kansas City Cardiomyopathy Questionnaire Score for improved quality of life at 2 years.For low-risk HF patients, pharmacist-led optimisation achieved significantly higher GDMT rates, reduced personnel healthcare costs, reduced GPs' workload, contributed to reduced cardiovascular mortality, reduced hospitalisations and improved quality of life. In the context of current workload pressures, this approach should be considered for widespread implementation in general practice.</p>\",\"PeriodicalId\":9052,\"journal\":{\"name\":\"BMJ Open Quality\",\"volume\":\"14 3\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406906/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Quality\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjoq-2025-003401\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2025-003401","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Pharmacist-led guideline-directed medical therapy in heart failure: impact analysis in primary care.
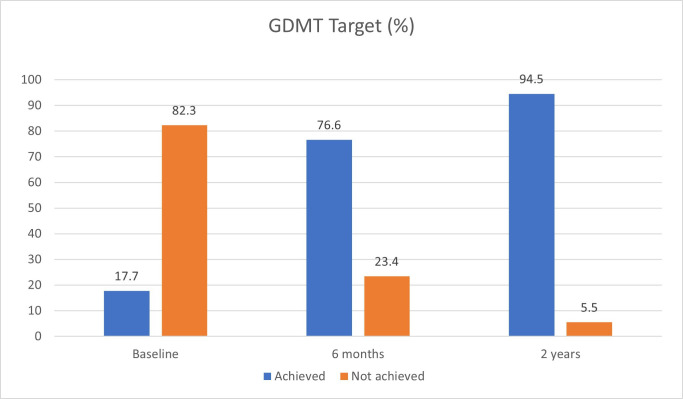
Optimal guideline-directed medical therapy (GDMT) can reduce mortality, unplanned hospital admissions and improve quality of life for patients suffering from heart failure (HF). However, GDMT remains underused in primary care. Only a minority of patients on HF registers receive optimal GDMT in the UK. This suboptimal care is compounded by a mounting lack of GP capacity and the growing burden of HF.A multisite, quantitative impact analysis was undertaken to evaluate the optimisation of HF patients by a novel pharmacist-led GDMT model in UK primary care.We identified low-risk HF patients suitable for pharmacists' input, including a community validated risk stratification tool-the HF Event STrengthening Score. The primary outcome was to compare the proportion of patients on optimal HF GDMT at 6 months and 2 years with baseline. Secondary outcomes were direct personnel healthcare costs and GP workload. A subgroup analysis was modelled to estimate effect on mortality, hospitalisation and quality of life.A total of 237 patients were included. Pharmacist-led GDMT contributed to the increase of optimal GDMT from 17.7% at baseline to 76.5% at 6 months and 94.5% at 2 years follow-up. The novel approach reduced GPs' HF GDMT workload by 36.6% at 6 months and 42.1% at 2 years and healthcare costs by 18.4% at 6 months and 20.3% at 2 years. Patients with combined angiotensin receptor neprilysin inhibitor/sodium glucose co-transporter 2 inhibitor treatment indicated a reduction of 20.8% in cardiovascular mortality, a reduction of 34.8% in hospitalisations and a 5.31 Kansas City Cardiomyopathy Questionnaire Score for improved quality of life at 2 years.For low-risk HF patients, pharmacist-led optimisation achieved significantly higher GDMT rates, reduced personnel healthcare costs, reduced GPs' workload, contributed to reduced cardiovascular mortality, reduced hospitalisations and improved quality of life. In the context of current workload pressures, this approach should be considered for widespread implementation in general practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


