{"title":"急诊科急性腹痛诊断路径的实施。","authors":"Samari Blomerus, Tracy-Lee Splinter, Amy Gillis, Orla Buckley, Hannah Turner, Aileen McCabe","doi":"10.1136/bmjoq-2025-003505","DOIUrl":null,"url":null,"abstract":"<p><p>Acute abdominal pain is a common acute presentation to the emergency department (ED). Contrast-enhanced abdominopelvic CT (AP CT) is typically the most appropriate imaging test. Previously in our ED, it was noted that the process to access AP CT was complicated and associated with delays. We implemented a quality intervention project to develop and implement a diagnostic pathway of ED patients with acute abdominal pain requiring AP CT imaging. Our overall aim was to improve ED length of stay and ED process times for patients presenting with acute abdominal pathology to our ED.After baseline data collection, we conducted a phased improvement project with pre-measurement and post-measurement. A rationalised multidisciplinary diagnostic pathway was agreed by the radiology, general surgery and emergency medicine teams. The imaging protocol for AP CT abdomens was revised using intravenous contrast only for the majority of patients. The ED length of stay statistically significantly improved from the pre-implementation period (1532 min), the first evaluation (1312 min) and the second evaluation period (1216 min) (p value<0.01). There was a non-statistically significant improvement in the mean-time from ED arrival to AP CT scan in the pre-implementation and post implementation phases (855 min in pre-implementation phase and 670 min and 621 min in the first and second phases, respectively, p=0.06). The overall positivity for significant acute pathology on CT abdomen in the implementation loop was 79.6%.The introduction of an acute abdominal pain diagnostic pathway improved ED throughput times and reduced admission rates in patients presenting to the ED with acute abdominal pain. The high diagnostic yield from AP CT scans indicates that our pathway was appropriate for ED patients with undifferentiated acute abdominal pain requiring urgent advanced imaging.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"14 3","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366589/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation of an acute abdominal pain diagnostic pathway in the emergency department.\",\"authors\":\"Samari Blomerus, Tracy-Lee Splinter, Amy Gillis, Orla Buckley, Hannah Turner, Aileen McCabe\",\"doi\":\"10.1136/bmjoq-2025-003505\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acute abdominal pain is a common acute presentation to the emergency department (ED). Contrast-enhanced abdominopelvic CT (AP CT) is typically the most appropriate imaging test. Previously in our ED, it was noted that the process to access AP CT was complicated and associated with delays. We implemented a quality intervention project to develop and implement a diagnostic pathway of ED patients with acute abdominal pain requiring AP CT imaging. Our overall aim was to improve ED length of stay and ED process times for patients presenting with acute abdominal pathology to our ED.After baseline data collection, we conducted a phased improvement project with pre-measurement and post-measurement. A rationalised multidisciplinary diagnostic pathway was agreed by the radiology, general surgery and emergency medicine teams. The imaging protocol for AP CT abdomens was revised using intravenous contrast only for the majority of patients. The ED length of stay statistically significantly improved from the pre-implementation period (1532 min), the first evaluation (1312 min) and the second evaluation period (1216 min) (p value<0.01). There was a non-statistically significant improvement in the mean-time from ED arrival to AP CT scan in the pre-implementation and post implementation phases (855 min in pre-implementation phase and 670 min and 621 min in the first and second phases, respectively, p=0.06). The overall positivity for significant acute pathology on CT abdomen in the implementation loop was 79.6%.The introduction of an acute abdominal pain diagnostic pathway improved ED throughput times and reduced admission rates in patients presenting to the ED with acute abdominal pain. The high diagnostic yield from AP CT scans indicates that our pathway was appropriate for ED patients with undifferentiated acute abdominal pain requiring urgent advanced imaging.</p>\",\"PeriodicalId\":9052,\"journal\":{\"name\":\"BMJ Open Quality\",\"volume\":\"14 3\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366589/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Quality\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjoq-2025-003505\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2025-003505","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Implementation of an acute abdominal pain diagnostic pathway in the emergency department.
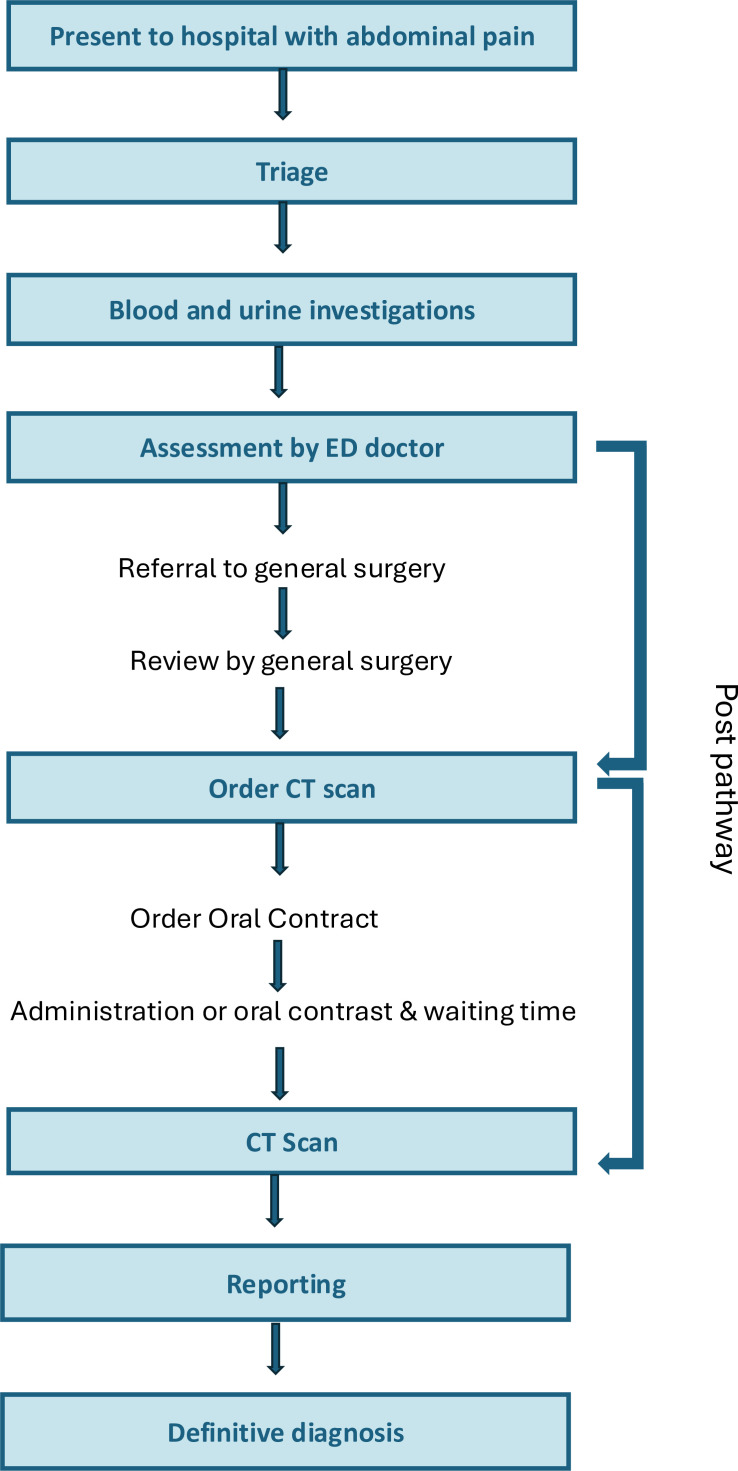
Acute abdominal pain is a common acute presentation to the emergency department (ED). Contrast-enhanced abdominopelvic CT (AP CT) is typically the most appropriate imaging test. Previously in our ED, it was noted that the process to access AP CT was complicated and associated with delays. We implemented a quality intervention project to develop and implement a diagnostic pathway of ED patients with acute abdominal pain requiring AP CT imaging. Our overall aim was to improve ED length of stay and ED process times for patients presenting with acute abdominal pathology to our ED.After baseline data collection, we conducted a phased improvement project with pre-measurement and post-measurement. A rationalised multidisciplinary diagnostic pathway was agreed by the radiology, general surgery and emergency medicine teams. The imaging protocol for AP CT abdomens was revised using intravenous contrast only for the majority of patients. The ED length of stay statistically significantly improved from the pre-implementation period (1532 min), the first evaluation (1312 min) and the second evaluation period (1216 min) (p value<0.01). There was a non-statistically significant improvement in the mean-time from ED arrival to AP CT scan in the pre-implementation and post implementation phases (855 min in pre-implementation phase and 670 min and 621 min in the first and second phases, respectively, p=0.06). The overall positivity for significant acute pathology on CT abdomen in the implementation loop was 79.6%.The introduction of an acute abdominal pain diagnostic pathway improved ED throughput times and reduced admission rates in patients presenting to the ED with acute abdominal pain. The high diagnostic yield from AP CT scans indicates that our pathway was appropriate for ED patients with undifferentiated acute abdominal pain requiring urgent advanced imaging.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


