Colin M McCrimmon, Molly R Fensterwald, Linda K Czypinski, Marc R Nuwer, Sherrille E Abelon, Melissa Reider-Demer
{"title":"通过神经病学和医学服务的标准化出院途径,加强病人流动。","authors":"Colin M McCrimmon, Molly R Fensterwald, Linda K Czypinski, Marc R Nuwer, Sherrille E Abelon, Melissa Reider-Demer","doi":"10.1136/bmjoq-2024-003303","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Poor discharge planning impairs hospital throughput, adds to the financial strain on health systems and diminishes patient and provider satisfaction. We developed consensus-based discharge criteria coupled with a standardised discharge pathway for four presenting diagnoses and tracked their effect on discharge timing and length of stay (LOS).</p><p><strong>Methods: </strong>Medical readiness for discharge criteria for patients diagnosed with transient ischaemic attack, seizure, demyelinating disease or syncope were generated by expert consensus at our institution. A standardised discharge pathway was developed for eligible patients based on discussions with stakeholders and staff. Discharge timing and readmissions were tracked for 6 months pre-intervention and 12 months post-intervention (divided into 6 months of implementation and post-implementation periods). The primary outcome was a discharge time of ≤2 hours for 60% of patients during the implementation period. Secondary outcomes included reduced time to discharge (TTD) and LOS compared with the pre-intervention period.</p><p><strong>Results: </strong>318 total patient visits were included across the baseline, implementation and post-implementation periods. Median TTD improved from 171 min at baseline to 88 and 92 min, respectively, during the implementation and post-implementation periods. Median LOS similarly decreased from 94 hours to 35 and 30 hours, respectively. All primary and secondary outcomes were achieved during the implementation period and sustained post-implementation. The rate of emergency department visits and hospital readmissions within 30 days remained low (~1.5%) post-intervention. Additionally, most providers reported that the intervention improved clinical workflow.</p><p><strong>Conclusions: </strong>This standardised discharge framework improved discharge efficiency for patients with four common diagnoses during an 18-month quality improvement study. The framework and its implementation are highly scalable, and similar systems-level approaches should be considered by hospitals to improve throughput.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"14 3","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374623/pdf/","citationCount":"0","resultStr":"{\"title\":\"Enhancing patient flow through standardised discharge pathways for neurology and medicine services.\",\"authors\":\"Colin M McCrimmon, Molly R Fensterwald, Linda K Czypinski, Marc R Nuwer, Sherrille E Abelon, Melissa Reider-Demer\",\"doi\":\"10.1136/bmjoq-2024-003303\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Poor discharge planning impairs hospital throughput, adds to the financial strain on health systems and diminishes patient and provider satisfaction. We developed consensus-based discharge criteria coupled with a standardised discharge pathway for four presenting diagnoses and tracked their effect on discharge timing and length of stay (LOS).</p><p><strong>Methods: </strong>Medical readiness for discharge criteria for patients diagnosed with transient ischaemic attack, seizure, demyelinating disease or syncope were generated by expert consensus at our institution. A standardised discharge pathway was developed for eligible patients based on discussions with stakeholders and staff. Discharge timing and readmissions were tracked for 6 months pre-intervention and 12 months post-intervention (divided into 6 months of implementation and post-implementation periods). The primary outcome was a discharge time of ≤2 hours for 60% of patients during the implementation period. Secondary outcomes included reduced time to discharge (TTD) and LOS compared with the pre-intervention period.</p><p><strong>Results: </strong>318 total patient visits were included across the baseline, implementation and post-implementation periods. Median TTD improved from 171 min at baseline to 88 and 92 min, respectively, during the implementation and post-implementation periods. Median LOS similarly decreased from 94 hours to 35 and 30 hours, respectively. All primary and secondary outcomes were achieved during the implementation period and sustained post-implementation. The rate of emergency department visits and hospital readmissions within 30 days remained low (~1.5%) post-intervention. Additionally, most providers reported that the intervention improved clinical workflow.</p><p><strong>Conclusions: </strong>This standardised discharge framework improved discharge efficiency for patients with four common diagnoses during an 18-month quality improvement study. The framework and its implementation are highly scalable, and similar systems-level approaches should be considered by hospitals to improve throughput.</p>\",\"PeriodicalId\":9052,\"journal\":{\"name\":\"BMJ Open Quality\",\"volume\":\"14 3\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374623/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Quality\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjoq-2024-003303\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2024-003303","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Enhancing patient flow through standardised discharge pathways for neurology and medicine services.
Background and objectives: Poor discharge planning impairs hospital throughput, adds to the financial strain on health systems and diminishes patient and provider satisfaction. We developed consensus-based discharge criteria coupled with a standardised discharge pathway for four presenting diagnoses and tracked their effect on discharge timing and length of stay (LOS).
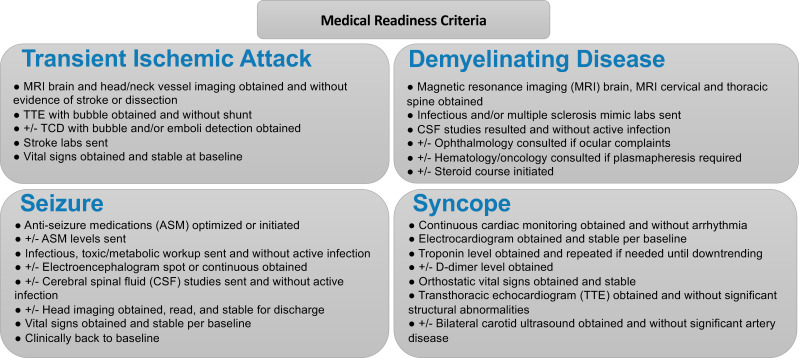
Methods: Medical readiness for discharge criteria for patients diagnosed with transient ischaemic attack, seizure, demyelinating disease or syncope were generated by expert consensus at our institution. A standardised discharge pathway was developed for eligible patients based on discussions with stakeholders and staff. Discharge timing and readmissions were tracked for 6 months pre-intervention and 12 months post-intervention (divided into 6 months of implementation and post-implementation periods). The primary outcome was a discharge time of ≤2 hours for 60% of patients during the implementation period. Secondary outcomes included reduced time to discharge (TTD) and LOS compared with the pre-intervention period.
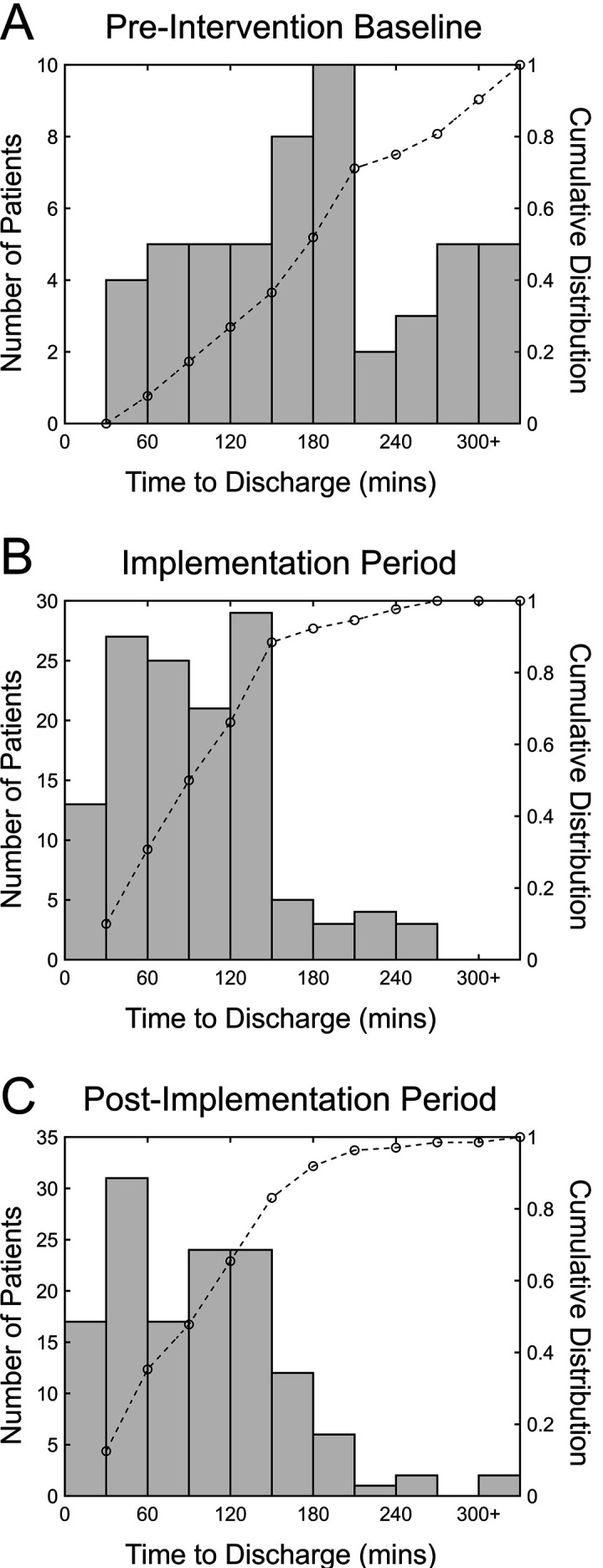
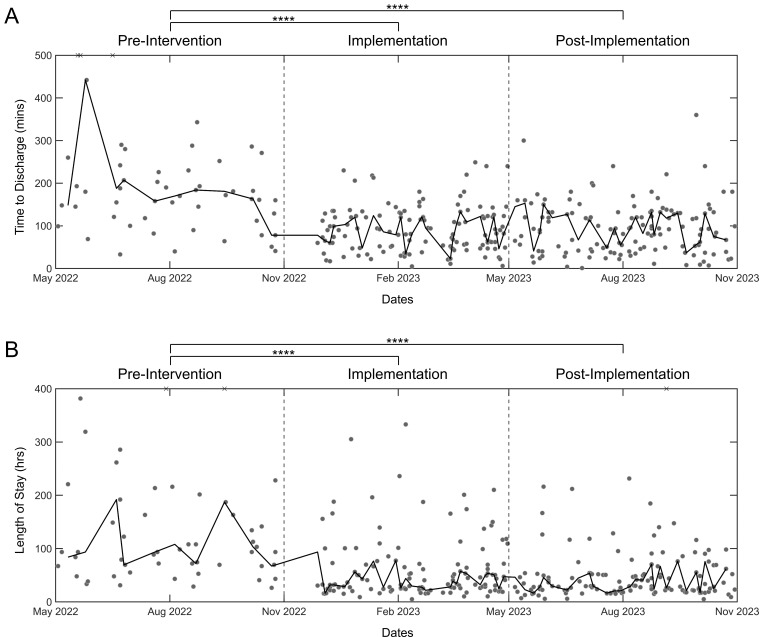
Results: 318 total patient visits were included across the baseline, implementation and post-implementation periods. Median TTD improved from 171 min at baseline to 88 and 92 min, respectively, during the implementation and post-implementation periods. Median LOS similarly decreased from 94 hours to 35 and 30 hours, respectively. All primary and secondary outcomes were achieved during the implementation period and sustained post-implementation. The rate of emergency department visits and hospital readmissions within 30 days remained low (~1.5%) post-intervention. Additionally, most providers reported that the intervention improved clinical workflow.
Conclusions: This standardised discharge framework improved discharge efficiency for patients with four common diagnoses during an 18-month quality improvement study. The framework and its implementation are highly scalable, and similar systems-level approaches should be considered by hospitals to improve throughput.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


