Mehdi Nasr Isfahani, Hamidreza Mohseni, Elahe Nasri Nasrabadi, Nizal Sarrafzadegan
{"title":"改进胸痛风险评估:验证HEART、TIMI、GRACE、EDACS-ADP和HET在急诊科的MACE预测","authors":"Mehdi Nasr Isfahani, Hamidreza Mohseni, Elahe Nasri Nasrabadi, Nizal Sarrafzadegan","doi":"10.1186/s12873-025-01327-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chest pain is a common and challenging complaint in emergency departments (EDs), necessitating accurate risk stratification to identify patients at risk for major adverse cardiac events (MACE) while avoiding unnecessary admissions. Several scoring systems have been developed for this purpose, yet their external validity in Middle Eastern populations remains understudied.</p><p><strong>Objective: </strong>To compare and validate the prognostic accuracy of HEART, TIMI, GRACE, EDACS-ADP, and HET scoring systems in predicting 6-week MACE among patients with chest pain presenting to two tertiary care centers in Isfahan, Iran.</p><p><strong>Methods: </strong>This retrospective cohort study included adult patients (aged > 18 years) who presented with non-traumatic chest pain to two tertiary referral centers in Isfahan between February and June 2024. Patients' clinical data, laboratory results, and electrocardiograms (ECGs) were retrieved to calculate standardized cardiac risk scores. The primary outcome was the occurrence of major adverse cardiac events (MACE) within 6 weeks following emergency department (ED) presentation. A 6-week evaluation window was selected based on institutional follow-up protocols, data availability, and existing literature that supports this timeframe as a critical period for early cardiac risk stratification. Diagnostic performance of the risk scores was evaluated using receiver operating characteristic (ROC) curve analysis, including calculation of sensitivity, specificity, positive and negative predictive values, and likelihood ratios at clinically relevant cut-off thresholds.</p><p><strong>Results: </strong>A total of 274 patients were finally included. Among them 68 (24.8%) met the MACE at presentation or within 6 weeks. The HEART score demonstrated the highest AUC: 0.925 and sensitivity: 97.1%; NPV: 98.18% at cut-off ≤ 3, followed closely by the HET score with AUC: 0.906 and sensitivity: 92.6%; NPV: 95.58% at cut-off ≤ 1. TIMI also performed well in identifying very low-risk patients (AUC: 0.868; sensitivity: 98.5%, NPV: 98.17%, though with limited specificity (26.7%). GRACE and EDACS-ADP showed moderate predictive ability, with AUCs of 0.815 and 0.803, respectively. Performance variations were attributed to differences in population demographics, and study design.</p><p><strong>Conclusion: </strong>The HEART and TIMI scores at the cut-offs of 3 and 1, respectively demonstrated superior discriminative ability in predicting 6-week MACE in this tertiary care cohort, supporting their use in ED settings for early discharge decisions. HET score also showed utility for ruling out MACE in high-risk patients, however, needs further validation due to its novelty and discrepancies observed among studies. These findings support the local implementation of HEART or TIMI in ED protocols, with further multicenter prospective validation recommended.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"165"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374469/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improving chest pain risk assessment: validation of HEART, TIMI, GRACE, EDACS-ADP, and HET for MACE prediction in the emergency department.\",\"authors\":\"Mehdi Nasr Isfahani, Hamidreza Mohseni, Elahe Nasri Nasrabadi, Nizal Sarrafzadegan\",\"doi\":\"10.1186/s12873-025-01327-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chest pain is a common and challenging complaint in emergency departments (EDs), necessitating accurate risk stratification to identify patients at risk for major adverse cardiac events (MACE) while avoiding unnecessary admissions. Several scoring systems have been developed for this purpose, yet their external validity in Middle Eastern populations remains understudied.</p><p><strong>Objective: </strong>To compare and validate the prognostic accuracy of HEART, TIMI, GRACE, EDACS-ADP, and HET scoring systems in predicting 6-week MACE among patients with chest pain presenting to two tertiary care centers in Isfahan, Iran.</p><p><strong>Methods: </strong>This retrospective cohort study included adult patients (aged > 18 years) who presented with non-traumatic chest pain to two tertiary referral centers in Isfahan between February and June 2024. Patients' clinical data, laboratory results, and electrocardiograms (ECGs) were retrieved to calculate standardized cardiac risk scores. The primary outcome was the occurrence of major adverse cardiac events (MACE) within 6 weeks following emergency department (ED) presentation. A 6-week evaluation window was selected based on institutional follow-up protocols, data availability, and existing literature that supports this timeframe as a critical period for early cardiac risk stratification. Diagnostic performance of the risk scores was evaluated using receiver operating characteristic (ROC) curve analysis, including calculation of sensitivity, specificity, positive and negative predictive values, and likelihood ratios at clinically relevant cut-off thresholds.</p><p><strong>Results: </strong>A total of 274 patients were finally included. Among them 68 (24.8%) met the MACE at presentation or within 6 weeks. The HEART score demonstrated the highest AUC: 0.925 and sensitivity: 97.1%; NPV: 98.18% at cut-off ≤ 3, followed closely by the HET score with AUC: 0.906 and sensitivity: 92.6%; NPV: 95.58% at cut-off ≤ 1. TIMI also performed well in identifying very low-risk patients (AUC: 0.868; sensitivity: 98.5%, NPV: 98.17%, though with limited specificity (26.7%). GRACE and EDACS-ADP showed moderate predictive ability, with AUCs of 0.815 and 0.803, respectively. Performance variations were attributed to differences in population demographics, and study design.</p><p><strong>Conclusion: </strong>The HEART and TIMI scores at the cut-offs of 3 and 1, respectively demonstrated superior discriminative ability in predicting 6-week MACE in this tertiary care cohort, supporting their use in ED settings for early discharge decisions. HET score also showed utility for ruling out MACE in high-risk patients, however, needs further validation due to its novelty and discrepancies observed among studies. These findings support the local implementation of HEART or TIMI in ED protocols, with further multicenter prospective validation recommended.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"25 1\",\"pages\":\"165\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374469/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-025-01327-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01327-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Improving chest pain risk assessment: validation of HEART, TIMI, GRACE, EDACS-ADP, and HET for MACE prediction in the emergency department.
Background: Chest pain is a common and challenging complaint in emergency departments (EDs), necessitating accurate risk stratification to identify patients at risk for major adverse cardiac events (MACE) while avoiding unnecessary admissions. Several scoring systems have been developed for this purpose, yet their external validity in Middle Eastern populations remains understudied.
Objective: To compare and validate the prognostic accuracy of HEART, TIMI, GRACE, EDACS-ADP, and HET scoring systems in predicting 6-week MACE among patients with chest pain presenting to two tertiary care centers in Isfahan, Iran.
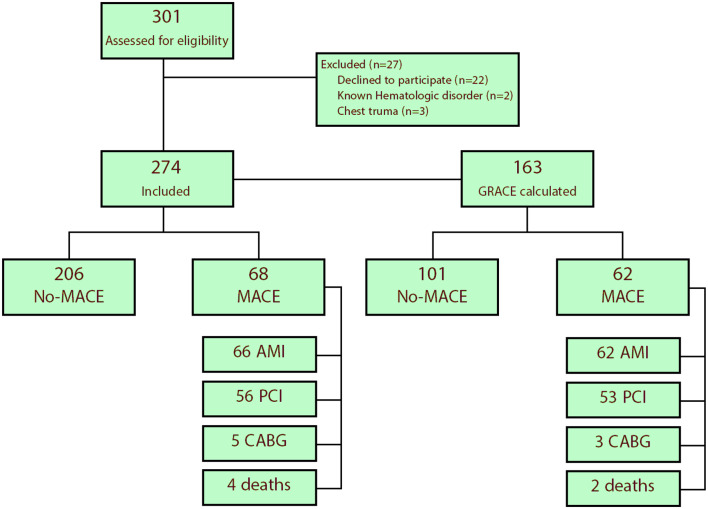
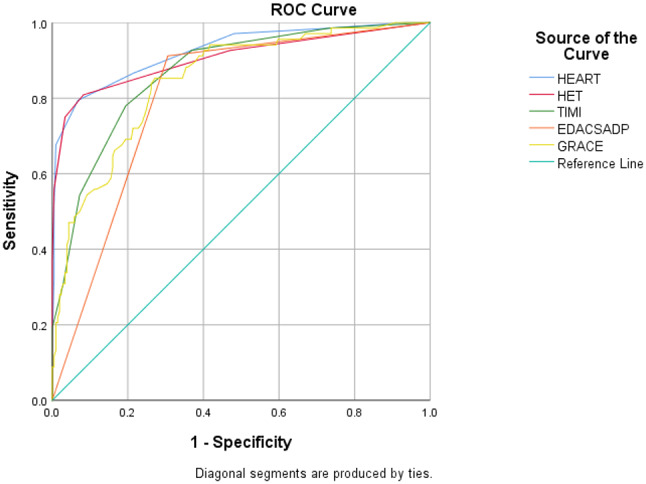
Methods: This retrospective cohort study included adult patients (aged > 18 years) who presented with non-traumatic chest pain to two tertiary referral centers in Isfahan between February and June 2024. Patients' clinical data, laboratory results, and electrocardiograms (ECGs) were retrieved to calculate standardized cardiac risk scores. The primary outcome was the occurrence of major adverse cardiac events (MACE) within 6 weeks following emergency department (ED) presentation. A 6-week evaluation window was selected based on institutional follow-up protocols, data availability, and existing literature that supports this timeframe as a critical period for early cardiac risk stratification. Diagnostic performance of the risk scores was evaluated using receiver operating characteristic (ROC) curve analysis, including calculation of sensitivity, specificity, positive and negative predictive values, and likelihood ratios at clinically relevant cut-off thresholds.
Results: A total of 274 patients were finally included. Among them 68 (24.8%) met the MACE at presentation or within 6 weeks. The HEART score demonstrated the highest AUC: 0.925 and sensitivity: 97.1%; NPV: 98.18% at cut-off ≤ 3, followed closely by the HET score with AUC: 0.906 and sensitivity: 92.6%; NPV: 95.58% at cut-off ≤ 1. TIMI also performed well in identifying very low-risk patients (AUC: 0.868; sensitivity: 98.5%, NPV: 98.17%, though with limited specificity (26.7%). GRACE and EDACS-ADP showed moderate predictive ability, with AUCs of 0.815 and 0.803, respectively. Performance variations were attributed to differences in population demographics, and study design.
Conclusion: The HEART and TIMI scores at the cut-offs of 3 and 1, respectively demonstrated superior discriminative ability in predicting 6-week MACE in this tertiary care cohort, supporting their use in ED settings for early discharge decisions. HET score also showed utility for ruling out MACE in high-risk patients, however, needs further validation due to its novelty and discrepancies observed among studies. These findings support the local implementation of HEART or TIMI in ED protocols, with further multicenter prospective validation recommended.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


