{"title":"阿片类药物治疗的风险变化及其与髋关节或膝关节置换术后死亡率的关联:基于14种不同定义的分析","authors":"Eskild Bendix Kristiansen, Alma B Pedersen","doi":"10.2340/17453674.2025.44572","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong> Long-term opioid therapy (LTOT) has frequently been reported in patients undergoing total hip or knee arthroplasty (THA or KA). However, there is no clear recommendation on the definition. We aimed to evaluate the sensitivity of the estimated risk of LTOT and association with mortality after THA and KA to the selection among 14 different candidate LTOT definitions.</p><p><strong>Methods: </strong> Using data from the nationwide Danish registries, we included patients with osteoarthritis undergoing primary THA during 2016-2019 (n = 28,957) or KA during 2014-2020 (n = 51,239). We obtained individual-level information on opioid prescriptions from any pharmacy 1 year before and 1 year after surgery. 14 common LTOT definitions were selected from the literature. The primary outcome was the variation in the 1-year crude risk of LTOT corresponding to variation in LTOT definition. Analysis was done overall and stratified by sex, age, prior opioid use, and year of surgery. The secondary outcome was the 4-year mortality among patients meeting each LTOT definition.</p><p><strong>Results: </strong> The 1-year risk of LTOT varied from 1.2% (95% confidence interval [CI] 1.1-1.3) to 20.1% (CI 19.6-20.5) for THA and 0.2% (CI 0.1-0.2) to 29.6% (CI 29.2-30.0) for KA patients depending on definition. For THA or KA, women had a higher risk of LTOT than men for all definitions, thus, LTOT varies from 0.2% (CI 0.1-0.2) to 32.9% (CI 32.3-33.4) for women and from 0.1% (CI 0.1-0.2) to 24.9% (24.4-25.5) for men. With increasing age risks of LTOT were steady or slightly decreasing. There was a decrease in the risk of LTOT from 2016 to 2019 for all definitions. 4-year mortality in patients meeting LTOT definitions varied from 9.8% (CI 8.9-10.7) to 16.3% (CI 13.2-20.1) for THA and 6.9% (CI 6.4-7.4) to 10.5% (CI 8.5-12.9) for KA patients.</p><p><strong>Conclusion: </strong> The estimation of the risk of LTOT after THA or KA and association with mortality is strongly dependent on the definition of LTOT used by researchers. This highlights the limitation on the comparability of opioid studies assessing risk and prognosis in these patients.</p>","PeriodicalId":6916,"journal":{"name":"Acta Orthopaedica","volume":"96 ","pages":"664-670"},"PeriodicalIF":2.4000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404099/pdf/","citationCount":"0","resultStr":"{\"title\":\"Variation in risk of opioid therapy and association with mortality following hip or knee arthroplasty: an analysis based on 14 different definitions.\",\"authors\":\"Eskild Bendix Kristiansen, Alma B Pedersen\",\"doi\":\"10.2340/17453674.2025.44572\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong> Long-term opioid therapy (LTOT) has frequently been reported in patients undergoing total hip or knee arthroplasty (THA or KA). However, there is no clear recommendation on the definition. We aimed to evaluate the sensitivity of the estimated risk of LTOT and association with mortality after THA and KA to the selection among 14 different candidate LTOT definitions.</p><p><strong>Methods: </strong> Using data from the nationwide Danish registries, we included patients with osteoarthritis undergoing primary THA during 2016-2019 (n = 28,957) or KA during 2014-2020 (n = 51,239). We obtained individual-level information on opioid prescriptions from any pharmacy 1 year before and 1 year after surgery. 14 common LTOT definitions were selected from the literature. The primary outcome was the variation in the 1-year crude risk of LTOT corresponding to variation in LTOT definition. Analysis was done overall and stratified by sex, age, prior opioid use, and year of surgery. The secondary outcome was the 4-year mortality among patients meeting each LTOT definition.</p><p><strong>Results: </strong> The 1-year risk of LTOT varied from 1.2% (95% confidence interval [CI] 1.1-1.3) to 20.1% (CI 19.6-20.5) for THA and 0.2% (CI 0.1-0.2) to 29.6% (CI 29.2-30.0) for KA patients depending on definition. For THA or KA, women had a higher risk of LTOT than men for all definitions, thus, LTOT varies from 0.2% (CI 0.1-0.2) to 32.9% (CI 32.3-33.4) for women and from 0.1% (CI 0.1-0.2) to 24.9% (24.4-25.5) for men. With increasing age risks of LTOT were steady or slightly decreasing. There was a decrease in the risk of LTOT from 2016 to 2019 for all definitions. 4-year mortality in patients meeting LTOT definitions varied from 9.8% (CI 8.9-10.7) to 16.3% (CI 13.2-20.1) for THA and 6.9% (CI 6.4-7.4) to 10.5% (CI 8.5-12.9) for KA patients.</p><p><strong>Conclusion: </strong> The estimation of the risk of LTOT after THA or KA and association with mortality is strongly dependent on the definition of LTOT used by researchers. This highlights the limitation on the comparability of opioid studies assessing risk and prognosis in these patients.</p>\",\"PeriodicalId\":6916,\"journal\":{\"name\":\"Acta Orthopaedica\",\"volume\":\"96 \",\"pages\":\"664-670\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404099/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Orthopaedica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2340/17453674.2025.44572\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Orthopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2340/17453674.2025.44572","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Variation in risk of opioid therapy and association with mortality following hip or knee arthroplasty: an analysis based on 14 different definitions.
Background and purpose: Long-term opioid therapy (LTOT) has frequently been reported in patients undergoing total hip or knee arthroplasty (THA or KA). However, there is no clear recommendation on the definition. We aimed to evaluate the sensitivity of the estimated risk of LTOT and association with mortality after THA and KA to the selection among 14 different candidate LTOT definitions.
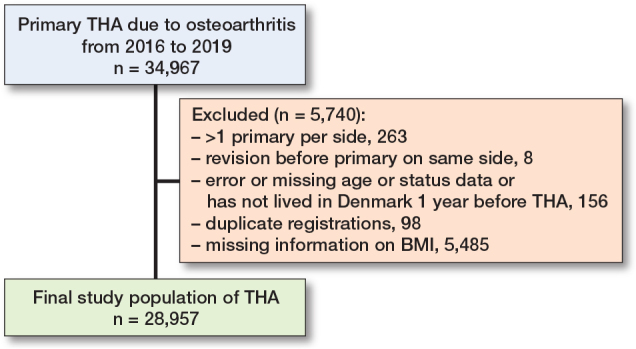
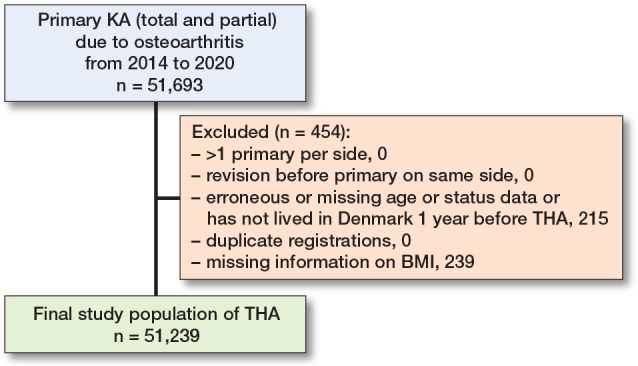
Methods: Using data from the nationwide Danish registries, we included patients with osteoarthritis undergoing primary THA during 2016-2019 (n = 28,957) or KA during 2014-2020 (n = 51,239). We obtained individual-level information on opioid prescriptions from any pharmacy 1 year before and 1 year after surgery. 14 common LTOT definitions were selected from the literature. The primary outcome was the variation in the 1-year crude risk of LTOT corresponding to variation in LTOT definition. Analysis was done overall and stratified by sex, age, prior opioid use, and year of surgery. The secondary outcome was the 4-year mortality among patients meeting each LTOT definition.
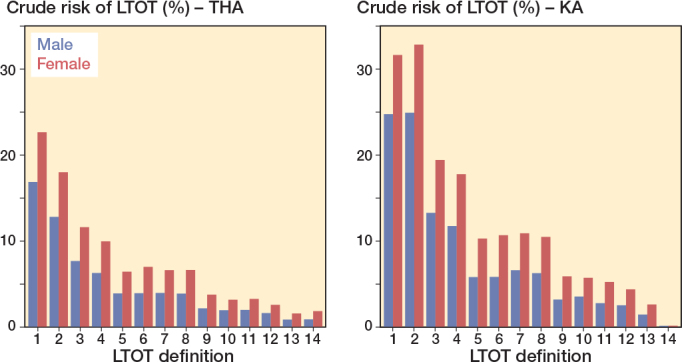
Results: The 1-year risk of LTOT varied from 1.2% (95% confidence interval [CI] 1.1-1.3) to 20.1% (CI 19.6-20.5) for THA and 0.2% (CI 0.1-0.2) to 29.6% (CI 29.2-30.0) for KA patients depending on definition. For THA or KA, women had a higher risk of LTOT than men for all definitions, thus, LTOT varies from 0.2% (CI 0.1-0.2) to 32.9% (CI 32.3-33.4) for women and from 0.1% (CI 0.1-0.2) to 24.9% (24.4-25.5) for men. With increasing age risks of LTOT were steady or slightly decreasing. There was a decrease in the risk of LTOT from 2016 to 2019 for all definitions. 4-year mortality in patients meeting LTOT definitions varied from 9.8% (CI 8.9-10.7) to 16.3% (CI 13.2-20.1) for THA and 6.9% (CI 6.4-7.4) to 10.5% (CI 8.5-12.9) for KA patients.
Conclusion: The estimation of the risk of LTOT after THA or KA and association with mortality is strongly dependent on the definition of LTOT used by researchers. This highlights the limitation on the comparability of opioid studies assessing risk and prognosis in these patients.
期刊介绍:
Acta Orthopaedica (previously Acta Orthopaedica Scandinavica) presents original articles of basic research interest, as well as clinical studies in the field of orthopedics and related sub disciplines. Ever since the journal was founded in 1930, by a group of Scandinavian orthopedic surgeons, the journal has been published for an international audience. Acta Orthopaedica is owned by the Nordic Orthopaedic Federation and is the official publication of this federation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


