Takuya Ogami MD , Ethan Chetkof BS , Johannes O. Bonatti MD , Christopher Pantelis BS , Stephen D. Waterford MD , Francis D. Ferdinand MD , Irsa S. Hasan MD , Derek Serna-Gallegos MD , David J. Kaczorowski MD , Danny Chu MD , Floyd W. Thoma BS , Ibrahim Sultan MD
{"title":"二尖瓣修复后小叶重建:切除与尊重策略重要吗?","authors":"Takuya Ogami MD , Ethan Chetkof BS , Johannes O. Bonatti MD , Christopher Pantelis BS , Stephen D. Waterford MD , Francis D. Ferdinand MD , Irsa S. Hasan MD , Derek Serna-Gallegos MD , David J. Kaczorowski MD , Danny Chu MD , Floyd W. Thoma BS , Ibrahim Sultan MD","doi":"10.1016/j.xjon.2025.06.009","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Previous randomized controlled trials demonstrated comparable outcomes between posterior leaflet resections and neochord implantation in mitral valve (MV) repair. However, these studies were limited up to 1-year follow-up, and more recent evidence suggested that leaflet resections may offer superior long-term outcomes.</div></div><div><h3>Methods</h3><div>All patients who underwent MV repair with either resection or neochord implantation for posterior leaflet pathology between October 2011 and July 2024 were included. Propensity-score matching was used.</div></div><div><h3>Results</h3><div>A total of 457 patients underwent posterior leaflet reconstruction, with 334 (73.1%) requiring leaflet resection (resection group) and 123 (26.9%) receiving neochordae (neochord group). The median [interquartile range] follow-up for survival and reintervention was 5.93 [2.00, 9.09] and 5.48 [1.84, 9.02] years, respectively. Overall, the mean age was 63.9 years, and the mean ejection fraction was 58.9%. Robotic-assisted surgery was performed in 28.9% (n = 132). The 30-day mortality was 2.4% (n = 11). Propensity-score matching provided 119 patients in each group. Kaplan-Meier curves demonstrated similar survival at 5 years between these groups (93.1 ± 2.8% in the resection group and 89.6 ± 3.1% in the neochord group, <em>P</em> = .5). However, the neochord group had a greater cumulative incidence of reoperative MV surgery (8.0% vs 0.9% at 5 years in the resection group, <em>P</em> = .01).</div></div><div><h3>Conclusions</h3><div>Neochordae were implanted in 27.3% of patients undergoing MV repair. Neochord implantation was associated with a greater risk of MV reintervention in the long term. Careful patient selection and technical considerations are important when choosing the repair method.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"26 ","pages":"Pages 94-103"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Posterior leaflet reconstruction in mitral valve repair: Does resect versus respect strategy matter?\",\"authors\":\"Takuya Ogami MD , Ethan Chetkof BS , Johannes O. Bonatti MD , Christopher Pantelis BS , Stephen D. Waterford MD , Francis D. Ferdinand MD , Irsa S. Hasan MD , Derek Serna-Gallegos MD , David J. Kaczorowski MD , Danny Chu MD , Floyd W. Thoma BS , Ibrahim Sultan MD\",\"doi\":\"10.1016/j.xjon.2025.06.009\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><div>Previous randomized controlled trials demonstrated comparable outcomes between posterior leaflet resections and neochord implantation in mitral valve (MV) repair. However, these studies were limited up to 1-year follow-up, and more recent evidence suggested that leaflet resections may offer superior long-term outcomes.</div></div><div><h3>Methods</h3><div>All patients who underwent MV repair with either resection or neochord implantation for posterior leaflet pathology between October 2011 and July 2024 were included. Propensity-score matching was used.</div></div><div><h3>Results</h3><div>A total of 457 patients underwent posterior leaflet reconstruction, with 334 (73.1%) requiring leaflet resection (resection group) and 123 (26.9%) receiving neochordae (neochord group). The median [interquartile range] follow-up for survival and reintervention was 5.93 [2.00, 9.09] and 5.48 [1.84, 9.02] years, respectively. Overall, the mean age was 63.9 years, and the mean ejection fraction was 58.9%. Robotic-assisted surgery was performed in 28.9% (n = 132). The 30-day mortality was 2.4% (n = 11). Propensity-score matching provided 119 patients in each group. Kaplan-Meier curves demonstrated similar survival at 5 years between these groups (93.1 ± 2.8% in the resection group and 89.6 ± 3.1% in the neochord group, <em>P</em> = .5). However, the neochord group had a greater cumulative incidence of reoperative MV surgery (8.0% vs 0.9% at 5 years in the resection group, <em>P</em> = .01).</div></div><div><h3>Conclusions</h3><div>Neochordae were implanted in 27.3% of patients undergoing MV repair. Neochord implantation was associated with a greater risk of MV reintervention in the long term. Careful patient selection and technical considerations are important when choosing the repair method.</div></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"26 \",\"pages\":\"Pages 94-103\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273625002153\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273625002153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
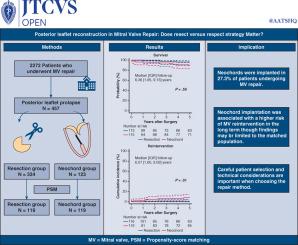
Posterior leaflet reconstruction in mitral valve repair: Does resect versus respect strategy matter?
Objective
Previous randomized controlled trials demonstrated comparable outcomes between posterior leaflet resections and neochord implantation in mitral valve (MV) repair. However, these studies were limited up to 1-year follow-up, and more recent evidence suggested that leaflet resections may offer superior long-term outcomes.
Methods
All patients who underwent MV repair with either resection or neochord implantation for posterior leaflet pathology between October 2011 and July 2024 were included. Propensity-score matching was used.
Results
A total of 457 patients underwent posterior leaflet reconstruction, with 334 (73.1%) requiring leaflet resection (resection group) and 123 (26.9%) receiving neochordae (neochord group). The median [interquartile range] follow-up for survival and reintervention was 5.93 [2.00, 9.09] and 5.48 [1.84, 9.02] years, respectively. Overall, the mean age was 63.9 years, and the mean ejection fraction was 58.9%. Robotic-assisted surgery was performed in 28.9% (n = 132). The 30-day mortality was 2.4% (n = 11). Propensity-score matching provided 119 patients in each group. Kaplan-Meier curves demonstrated similar survival at 5 years between these groups (93.1 ± 2.8% in the resection group and 89.6 ± 3.1% in the neochord group, P = .5). However, the neochord group had a greater cumulative incidence of reoperative MV surgery (8.0% vs 0.9% at 5 years in the resection group, P = .01).
Conclusions
Neochordae were implanted in 27.3% of patients undergoing MV repair. Neochord implantation was associated with a greater risk of MV reintervention in the long term. Careful patient selection and technical considerations are important when choosing the repair method.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


