Anna Olds MD, MS , James M. Meza MD, MS , Nithya Rajeev BS , Mike Kim BS , Luke M. Wiggins MD , Winfield J. Wells MD , Vaughn A. Starnes MD , John David Cleveland MD
{"title":"异位相关先天性心脏病复杂而危险的病程","authors":"Anna Olds MD, MS , James M. Meza MD, MS , Nithya Rajeev BS , Mike Kim BS , Luke M. Wiggins MD , Winfield J. Wells MD , Vaughn A. Starnes MD , John David Cleveland MD","doi":"10.1016/j.xjon.2025.06.018","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Patients with heterotaxy-associated congenital heart disease often require multiple operations, which may have a cumulative effect on their outcomes. This study aimed to define the cardiac surgical course in a large cohort and identify longitudinal risk factors for death/transplant.</div></div><div><h3>Methods</h3><div>All patients with heterotaxy-associated congenital heart disease who underwent cardiac surgery at one institution from 2005 to 2022 were retrospectively reviewed. Demographics, anatomy, and operative course were summarized. Parametric risk hazard analysis for death/transplant was performed. Operations were analyzed as time-varying covariates.</div></div><div><h3>Results</h3><div>Of 217 patients included, left isomerism occurred in 89 (41%), 139 (64%) were right ventricle dominant, and 43 (20%) had biventricular dominance. Total anomalous pulmonary venous return occurred in 100 patients (46%): 40 (40%) supracardiac, 34 (34%) intracardiac, 18 (18%) infracardiac, 7 (7%) mixed, and 19 (19%) obstructed. Ultimately, 102 patients (47%) reached the Fontan and 29 patients (13%) reached biventricular circulation. Transplant-free survivals at 1, 5, and 10 years were 79.4% ± 3%, 71.0% ± 3%, 63.9% ± 3%, respectively. Multivariable parametric analysis resolved 2 phases of risk for death/transplant. First-phase predictors included coarctation (parameter estimate 0.91 ± 0.55, <em>P = .</em>04) and time-varying total anomalous pulmonary venous return repair + pulmonary blood flow control (parameter estimate 1.64 ± 0.37, <em>P < .</em>001). Second-phase predictors included tricuspid atresia (parameter estimate 2.17 ± 0.59, <em>P < .</em>001), time-varying Fontan revision (parameter estimate 3.48 ± 0.51, <em>P < .</em>001), and time-varying atrioventricular valve repair/replacement (3.55 ± 0.54, <em>P < .</em>001). Reaching the Glenn reduced the risk of death/transplant (parameter estimate −1.85 ± 0.54, <em>P < .</em>001).</div></div><div><h3>Conclusions</h3><div>Operative management of heterotaxy-associated congenital heart disease is high risk, especially when total anomalous pulmonary venous return repair with pulmonary blood flow control is required. Risk after infancy is primarily determined by need for the Fontan or atrioventricular valve reintervention.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"26 ","pages":"Pages 196-206"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"The complex and hazardous course for heterotaxy-associated congenital heart disease\",\"authors\":\"Anna Olds MD, MS , James M. Meza MD, MS , Nithya Rajeev BS , Mike Kim BS , Luke M. Wiggins MD , Winfield J. Wells MD , Vaughn A. Starnes MD , John David Cleveland MD\",\"doi\":\"10.1016/j.xjon.2025.06.018\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><div>Patients with heterotaxy-associated congenital heart disease often require multiple operations, which may have a cumulative effect on their outcomes. This study aimed to define the cardiac surgical course in a large cohort and identify longitudinal risk factors for death/transplant.</div></div><div><h3>Methods</h3><div>All patients with heterotaxy-associated congenital heart disease who underwent cardiac surgery at one institution from 2005 to 2022 were retrospectively reviewed. Demographics, anatomy, and operative course were summarized. Parametric risk hazard analysis for death/transplant was performed. Operations were analyzed as time-varying covariates.</div></div><div><h3>Results</h3><div>Of 217 patients included, left isomerism occurred in 89 (41%), 139 (64%) were right ventricle dominant, and 43 (20%) had biventricular dominance. Total anomalous pulmonary venous return occurred in 100 patients (46%): 40 (40%) supracardiac, 34 (34%) intracardiac, 18 (18%) infracardiac, 7 (7%) mixed, and 19 (19%) obstructed. Ultimately, 102 patients (47%) reached the Fontan and 29 patients (13%) reached biventricular circulation. Transplant-free survivals at 1, 5, and 10 years were 79.4% ± 3%, 71.0% ± 3%, 63.9% ± 3%, respectively. Multivariable parametric analysis resolved 2 phases of risk for death/transplant. First-phase predictors included coarctation (parameter estimate 0.91 ± 0.55, <em>P = .</em>04) and time-varying total anomalous pulmonary venous return repair + pulmonary blood flow control (parameter estimate 1.64 ± 0.37, <em>P < .</em>001). Second-phase predictors included tricuspid atresia (parameter estimate 2.17 ± 0.59, <em>P < .</em>001), time-varying Fontan revision (parameter estimate 3.48 ± 0.51, <em>P < .</em>001), and time-varying atrioventricular valve repair/replacement (3.55 ± 0.54, <em>P < .</em>001). Reaching the Glenn reduced the risk of death/transplant (parameter estimate −1.85 ± 0.54, <em>P < .</em>001).</div></div><div><h3>Conclusions</h3><div>Operative management of heterotaxy-associated congenital heart disease is high risk, especially when total anomalous pulmonary venous return repair with pulmonary blood flow control is required. Risk after infancy is primarily determined by need for the Fontan or atrioventricular valve reintervention.</div></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"26 \",\"pages\":\"Pages 196-206\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273625002244\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273625002244","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
The complex and hazardous course for heterotaxy-associated congenital heart disease
Objective
Patients with heterotaxy-associated congenital heart disease often require multiple operations, which may have a cumulative effect on their outcomes. This study aimed to define the cardiac surgical course in a large cohort and identify longitudinal risk factors for death/transplant.
Methods
All patients with heterotaxy-associated congenital heart disease who underwent cardiac surgery at one institution from 2005 to 2022 were retrospectively reviewed. Demographics, anatomy, and operative course were summarized. Parametric risk hazard analysis for death/transplant was performed. Operations were analyzed as time-varying covariates.
Results
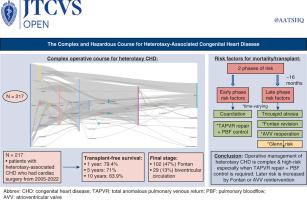
Of 217 patients included, left isomerism occurred in 89 (41%), 139 (64%) were right ventricle dominant, and 43 (20%) had biventricular dominance. Total anomalous pulmonary venous return occurred in 100 patients (46%): 40 (40%) supracardiac, 34 (34%) intracardiac, 18 (18%) infracardiac, 7 (7%) mixed, and 19 (19%) obstructed. Ultimately, 102 patients (47%) reached the Fontan and 29 patients (13%) reached biventricular circulation. Transplant-free survivals at 1, 5, and 10 years were 79.4% ± 3%, 71.0% ± 3%, 63.9% ± 3%, respectively. Multivariable parametric analysis resolved 2 phases of risk for death/transplant. First-phase predictors included coarctation (parameter estimate 0.91 ± 0.55, P = .04) and time-varying total anomalous pulmonary venous return repair + pulmonary blood flow control (parameter estimate 1.64 ± 0.37, P < .001). Second-phase predictors included tricuspid atresia (parameter estimate 2.17 ± 0.59, P < .001), time-varying Fontan revision (parameter estimate 3.48 ± 0.51, P < .001), and time-varying atrioventricular valve repair/replacement (3.55 ± 0.54, P < .001). Reaching the Glenn reduced the risk of death/transplant (parameter estimate −1.85 ± 0.54, P < .001).
Conclusions
Operative management of heterotaxy-associated congenital heart disease is high risk, especially when total anomalous pulmonary venous return repair with pulmonary blood flow control is required. Risk after infancy is primarily determined by need for the Fontan or atrioventricular valve reintervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


