Joshua D. Sparks MD , Sarah J. Wilkens MD , Andrea Nicole Lambert MD , Deborah Kozik DO , Jaimin R. Trivedi MBBS, MPH , Bahaaldin Alsoufi MD
{"title":"严重肥胖增加儿童心脏移植中移植物丢失的风险","authors":"Joshua D. Sparks MD , Sarah J. Wilkens MD , Andrea Nicole Lambert MD , Deborah Kozik DO , Jaimin R. Trivedi MBBS, MPH , Bahaaldin Alsoufi MD","doi":"10.1016/j.xjon.2025.04.023","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>Severe obesity is an established risk factor for adverse cardiovascular events and heart transplantation (HT) outcomes in adults. However, the effect of severe obesity on children after HT is not well studied. We aimed to examine the prevalence and effect of severe obesity on pediatric HT.</div></div><div><h3>Methods</h3><div>We evaluated children (>8 years) listed for HT using the United Network for Organ Sharing database. Severe obesity was defined per Centers for Disease Control and Prevention criteria using body mass index. Our study comprised 2 groups: a severe obesity group (n = 212, 8%) and a control group (n = 2417, 92%) consisting of the remaining children. We compared characteristics and outcomes between the 2 groups.</div></div><div><h3>Results</h3><div>After listing, there was no difference in transplant rate or waitlist mortality between the severe obesity and control groups (<em>P</em> = .89). Children with severe obesity were less likely to have congenital heart disease and more likely to be Black, have greater levels of creatinine, be supported with a left ventricular assist device, and receive grafts from older donors. Waitlist duration was comparable (<em>P</em> = .23). Incidences of primary graft dysfunction (<em>P</em> = .91), stroke (<em>P</em> = .36), dialysis (<em>P</em> = .18), and acute rejection (<em>P</em> = .4) were similar. However, severe obesity group had significant survival disadvantage (10 years: 47% vs 64%, <em>P</em> = .01), particularly in children older than 11 years, with diverging outcomes starting around 4 years posttransplant in those older than 15 years. Cox regression identified severe obesity as independent mortality risk factor (hazard ratio, 1.88; <em>P</em> = .0003), along with age, gender, race, congenital heart disease, creatinine, extracorporeal membrane oxygenation, and donor age.</div></div><div><h3>Conclusions</h3><div>There is a pressing need to improve assessment and treatment of obesity in children with end-stage heart failure awaiting transplantation. Although early survival rates are comparable, med- and long-term outcomes are concerning for severely obese children after heart transplant. Though unclear, the pathophysiologic effects are likely due to accelerated allograft vasculopathy from the metabolic derangement of obesity. Particularly in older children and adolescents, severe obesity should be considered a modifiable risk factor and aggressively managed before and after transplantation.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"26 ","pages":"Pages 207-217"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Severe obesity increases risk of graft loss in pediatric heart transplantation\",\"authors\":\"Joshua D. Sparks MD , Sarah J. Wilkens MD , Andrea Nicole Lambert MD , Deborah Kozik DO , Jaimin R. Trivedi MBBS, MPH , Bahaaldin Alsoufi MD\",\"doi\":\"10.1016/j.xjon.2025.04.023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><div>Severe obesity is an established risk factor for adverse cardiovascular events and heart transplantation (HT) outcomes in adults. However, the effect of severe obesity on children after HT is not well studied. We aimed to examine the prevalence and effect of severe obesity on pediatric HT.</div></div><div><h3>Methods</h3><div>We evaluated children (>8 years) listed for HT using the United Network for Organ Sharing database. Severe obesity was defined per Centers for Disease Control and Prevention criteria using body mass index. Our study comprised 2 groups: a severe obesity group (n = 212, 8%) and a control group (n = 2417, 92%) consisting of the remaining children. We compared characteristics and outcomes between the 2 groups.</div></div><div><h3>Results</h3><div>After listing, there was no difference in transplant rate or waitlist mortality between the severe obesity and control groups (<em>P</em> = .89). Children with severe obesity were less likely to have congenital heart disease and more likely to be Black, have greater levels of creatinine, be supported with a left ventricular assist device, and receive grafts from older donors. Waitlist duration was comparable (<em>P</em> = .23). Incidences of primary graft dysfunction (<em>P</em> = .91), stroke (<em>P</em> = .36), dialysis (<em>P</em> = .18), and acute rejection (<em>P</em> = .4) were similar. However, severe obesity group had significant survival disadvantage (10 years: 47% vs 64%, <em>P</em> = .01), particularly in children older than 11 years, with diverging outcomes starting around 4 years posttransplant in those older than 15 years. Cox regression identified severe obesity as independent mortality risk factor (hazard ratio, 1.88; <em>P</em> = .0003), along with age, gender, race, congenital heart disease, creatinine, extracorporeal membrane oxygenation, and donor age.</div></div><div><h3>Conclusions</h3><div>There is a pressing need to improve assessment and treatment of obesity in children with end-stage heart failure awaiting transplantation. Although early survival rates are comparable, med- and long-term outcomes are concerning for severely obese children after heart transplant. Though unclear, the pathophysiologic effects are likely due to accelerated allograft vasculopathy from the metabolic derangement of obesity. Particularly in older children and adolescents, severe obesity should be considered a modifiable risk factor and aggressively managed before and after transplantation.</div></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"26 \",\"pages\":\"Pages 207-217\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273625001548\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273625001548","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
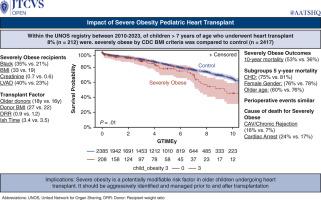
Severe obesity increases risk of graft loss in pediatric heart transplantation
Objectives
Severe obesity is an established risk factor for adverse cardiovascular events and heart transplantation (HT) outcomes in adults. However, the effect of severe obesity on children after HT is not well studied. We aimed to examine the prevalence and effect of severe obesity on pediatric HT.
Methods
We evaluated children (>8 years) listed for HT using the United Network for Organ Sharing database. Severe obesity was defined per Centers for Disease Control and Prevention criteria using body mass index. Our study comprised 2 groups: a severe obesity group (n = 212, 8%) and a control group (n = 2417, 92%) consisting of the remaining children. We compared characteristics and outcomes between the 2 groups.
Results
After listing, there was no difference in transplant rate or waitlist mortality between the severe obesity and control groups (P = .89). Children with severe obesity were less likely to have congenital heart disease and more likely to be Black, have greater levels of creatinine, be supported with a left ventricular assist device, and receive grafts from older donors. Waitlist duration was comparable (P = .23). Incidences of primary graft dysfunction (P = .91), stroke (P = .36), dialysis (P = .18), and acute rejection (P = .4) were similar. However, severe obesity group had significant survival disadvantage (10 years: 47% vs 64%, P = .01), particularly in children older than 11 years, with diverging outcomes starting around 4 years posttransplant in those older than 15 years. Cox regression identified severe obesity as independent mortality risk factor (hazard ratio, 1.88; P = .0003), along with age, gender, race, congenital heart disease, creatinine, extracorporeal membrane oxygenation, and donor age.
Conclusions
There is a pressing need to improve assessment and treatment of obesity in children with end-stage heart failure awaiting transplantation. Although early survival rates are comparable, med- and long-term outcomes are concerning for severely obese children after heart transplant. Though unclear, the pathophysiologic effects are likely due to accelerated allograft vasculopathy from the metabolic derangement of obesity. Particularly in older children and adolescents, severe obesity should be considered a modifiable risk factor and aggressively managed before and after transplantation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


