{"title":"无心包积液的室性无壁破裂:急性心肌梗死的诊断挑战","authors":"Ranin Hilu , Yoram Neuman , Abid Assali , Hana Vaknin Assa","doi":"10.1016/j.crmic.2025.100099","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Left ventricular free wall rupture is a rare but often fatal complication of acute myocardial infarction (MI). While typically associated with pericardial effusion and tamponade, left ventricular free wall rupture can occasionally present as a contained rupture, leading to diagnostic delays.</div></div><div><h3>Case summary</h3><div>A 69-year-old woman with prior mitral and tricuspid valve repair and atrial flutter treated with apixaban presented with cardiogenic shock following a posterior ST-elevation MI. Coronary angiography revealed thrombus in the right coronary artery and thrombotic occlusion of the left circumflex artery (LCx)- obtuse marginal (OM) branch. During evaluation for mechanical support, echocardiography suggested a large left ventricular mass. Further imaging raised suspicion of an intramural hematoma without pericardial effusion. Surgical exploration confirmed a sealed ventricular rupture contained by the parietal pericardium. Despite timely intervention, the patient succumbed to her condition.</div></div><div><h3>Discussion</h3><div>This case emphasizes the diagnostic challenge posed by left ventricular free wall rupture without pericardial effusion. High clinical suspicion, even in atypical presentations, and rapid multidisciplinary management are critical for improved outcomes.</div></div>","PeriodicalId":100217,"journal":{"name":"Cardiovascular Revascularization Medicine: Interesting Cases","volume":"9 ","pages":"Article 100099"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Contained ventricular free wall rupture without pericardial effusion: a diagnostic challenge in acute myocardial infarction\",\"authors\":\"Ranin Hilu , Yoram Neuman , Abid Assali , Hana Vaknin Assa\",\"doi\":\"10.1016/j.crmic.2025.100099\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><div>Left ventricular free wall rupture is a rare but often fatal complication of acute myocardial infarction (MI). While typically associated with pericardial effusion and tamponade, left ventricular free wall rupture can occasionally present as a contained rupture, leading to diagnostic delays.</div></div><div><h3>Case summary</h3><div>A 69-year-old woman with prior mitral and tricuspid valve repair and atrial flutter treated with apixaban presented with cardiogenic shock following a posterior ST-elevation MI. Coronary angiography revealed thrombus in the right coronary artery and thrombotic occlusion of the left circumflex artery (LCx)- obtuse marginal (OM) branch. During evaluation for mechanical support, echocardiography suggested a large left ventricular mass. Further imaging raised suspicion of an intramural hematoma without pericardial effusion. Surgical exploration confirmed a sealed ventricular rupture contained by the parietal pericardium. Despite timely intervention, the patient succumbed to her condition.</div></div><div><h3>Discussion</h3><div>This case emphasizes the diagnostic challenge posed by left ventricular free wall rupture without pericardial effusion. High clinical suspicion, even in atypical presentations, and rapid multidisciplinary management are critical for improved outcomes.</div></div>\",\"PeriodicalId\":100217,\"journal\":{\"name\":\"Cardiovascular Revascularization Medicine: Interesting Cases\",\"volume\":\"9 \",\"pages\":\"Article 100099\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular Revascularization Medicine: Interesting Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2950275625000450\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Revascularization Medicine: Interesting Cases","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2950275625000450","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Contained ventricular free wall rupture without pericardial effusion: a diagnostic challenge in acute myocardial infarction
Background
Left ventricular free wall rupture is a rare but often fatal complication of acute myocardial infarction (MI). While typically associated with pericardial effusion and tamponade, left ventricular free wall rupture can occasionally present as a contained rupture, leading to diagnostic delays.
Case summary
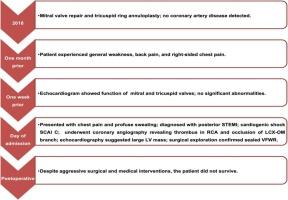
A 69-year-old woman with prior mitral and tricuspid valve repair and atrial flutter treated with apixaban presented with cardiogenic shock following a posterior ST-elevation MI. Coronary angiography revealed thrombus in the right coronary artery and thrombotic occlusion of the left circumflex artery (LCx)- obtuse marginal (OM) branch. During evaluation for mechanical support, echocardiography suggested a large left ventricular mass. Further imaging raised suspicion of an intramural hematoma without pericardial effusion. Surgical exploration confirmed a sealed ventricular rupture contained by the parietal pericardium. Despite timely intervention, the patient succumbed to her condition.
Discussion
This case emphasizes the diagnostic challenge posed by left ventricular free wall rupture without pericardial effusion. High clinical suspicion, even in atypical presentations, and rapid multidisciplinary management are critical for improved outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


