Daniel G Rayner, Darsh Shah, Si-Cheng Dai, David Gou, Jason Z X Chen, Arnav Agarwal, Reem A Mustafa, Veena Manja, Per Olav Vandvik, Thomas Agoritsas, Farid Foroutan
{"title":"2型糖尿病患者心血管和肾脏预后模型:观察性研究的实时系统回顾和荟萃分析","authors":"Daniel G Rayner, Darsh Shah, Si-Cheng Dai, David Gou, Jason Z X Chen, Arnav Agarwal, Reem A Mustafa, Veena Manja, Per Olav Vandvik, Thomas Agoritsas, Farid Foroutan","doi":"10.1136/bmjmed-2025-001369","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To summarise available evidence regarding the performance metrics of validated prognostic models on cardiovascular and kidney outcomes in adults with type 2 diabetes mellitus.</p><p><strong>Design: </strong>Living systematic review and meta-analysis of observational studies.</p><p><strong>Data sources: </strong>Medline, Embase, Central, and the Cochrane Database of Systematic Reviews from 1 January 2020 to 17 January 2024.</p><p><strong>Eligibility criteria for selecting studies: </strong>Studies validating prognostic models that predicted all cause and cardiovascular mortality, admission to hospital for heart failure, kidney failure, myocardial infarction, or ischaemic stroke in adults with type 2 diabetes mellitus, including people with established cardiovascular disease or chronic kidney disease, or both. Risk models evaluating composite outcomes were not eligible.</p><p><strong>Data synthesis: </strong>For each model and outcome, using a random effects model, the reported discrimination measures were pooled, reported as c statistics. Furthermore, when available, calibration plots were reconstructed and interpreted narratively. The Prediction Model Risk of Bias Assessment (PROBAST) tool was used to assess the risk of bias of each analysed study cohort and the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach to evaluate our certainty in the evidence.</p><p><strong>Results: </strong>6529 publications were identified, of which 35 studies reporting on 13 models were included, all of which were developed for general populations with type 2 diabetes but no established cardiovascular disease or chronic kidney disease. Among the identified models, the Risk Equations for Complications of Type 2 Diabetes (RECODe) and the UK Prospective Diabetes Study Outcomes Model 2 (UKPDS-OM2) evaluated all outcomes except for admission to hospital for heart failure. Relative to a threshold c statistic of 0.7, RECODe had an acceptable discrimination for cardiovascular mortality (0.79, high certainty), probably has an acceptable discrimination for myocardial infarction (0.72, moderate certainty) and stroke (0.71, moderate certainty), and may have an acceptable discrimination for kidney failure (0.76, low certainty). High certainty evidence suggests that UKPDS-OM2 has unacceptable discrimination for myocardial infarction (0.64) and stroke (0.65). RECODe showed acceptable calibration for cardiovascular mortality (high certainty), myocardial infarction (high certainty), and kidney failure (moderate certainty) but had unacceptable calibration for stroke (moderate certainty). UKPDS-OM2 showed acceptable calibration for cardiovascular mortality (moderate certainty), stroke (moderate certainty), and kidney failure (low certainty), but may have unacceptable calibration for myocardial infarction (moderate certainty).</p><p><strong>Conclusion: </strong>13 unique models were identified that evaluated cardiovascular and kidney outcomes in patients with type 2 diabetes. Two models, RECODe and UKPDS-OM2, evaluated all outcomes except for admission to hospital for heart failure. Of all the appraised prognostic models, RECODe had acceptable discrimination and calibration in validation studies for most outcomes; although, additional studies directly comparing models are needed.</p><p><strong>Study registration number: </strong>PROSPERO, CRD42023423075.</p><p><strong>Readers’ note: </strong>This article is a living systematic review that will be updated to reflect emerging evidence. Updates may occur for up to two years from the date of original publication. This version is the original article.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"4 1","pages":"e001369"},"PeriodicalIF":10.0000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359462/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic models for cardiovascular and kidney outcomes in people with type 2 diabetes: living systematic review and meta-analysis of observational studies.\",\"authors\":\"Daniel G Rayner, Darsh Shah, Si-Cheng Dai, David Gou, Jason Z X Chen, Arnav Agarwal, Reem A Mustafa, Veena Manja, Per Olav Vandvik, Thomas Agoritsas, Farid Foroutan\",\"doi\":\"10.1136/bmjmed-2025-001369\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To summarise available evidence regarding the performance metrics of validated prognostic models on cardiovascular and kidney outcomes in adults with type 2 diabetes mellitus.</p><p><strong>Design: </strong>Living systematic review and meta-analysis of observational studies.</p><p><strong>Data sources: </strong>Medline, Embase, Central, and the Cochrane Database of Systematic Reviews from 1 January 2020 to 17 January 2024.</p><p><strong>Eligibility criteria for selecting studies: </strong>Studies validating prognostic models that predicted all cause and cardiovascular mortality, admission to hospital for heart failure, kidney failure, myocardial infarction, or ischaemic stroke in adults with type 2 diabetes mellitus, including people with established cardiovascular disease or chronic kidney disease, or both. Risk models evaluating composite outcomes were not eligible.</p><p><strong>Data synthesis: </strong>For each model and outcome, using a random effects model, the reported discrimination measures were pooled, reported as c statistics. Furthermore, when available, calibration plots were reconstructed and interpreted narratively. The Prediction Model Risk of Bias Assessment (PROBAST) tool was used to assess the risk of bias of each analysed study cohort and the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach to evaluate our certainty in the evidence.</p><p><strong>Results: </strong>6529 publications were identified, of which 35 studies reporting on 13 models were included, all of which were developed for general populations with type 2 diabetes but no established cardiovascular disease or chronic kidney disease. Among the identified models, the Risk Equations for Complications of Type 2 Diabetes (RECODe) and the UK Prospective Diabetes Study Outcomes Model 2 (UKPDS-OM2) evaluated all outcomes except for admission to hospital for heart failure. Relative to a threshold c statistic of 0.7, RECODe had an acceptable discrimination for cardiovascular mortality (0.79, high certainty), probably has an acceptable discrimination for myocardial infarction (0.72, moderate certainty) and stroke (0.71, moderate certainty), and may have an acceptable discrimination for kidney failure (0.76, low certainty). High certainty evidence suggests that UKPDS-OM2 has unacceptable discrimination for myocardial infarction (0.64) and stroke (0.65). RECODe showed acceptable calibration for cardiovascular mortality (high certainty), myocardial infarction (high certainty), and kidney failure (moderate certainty) but had unacceptable calibration for stroke (moderate certainty). UKPDS-OM2 showed acceptable calibration for cardiovascular mortality (moderate certainty), stroke (moderate certainty), and kidney failure (low certainty), but may have unacceptable calibration for myocardial infarction (moderate certainty).</p><p><strong>Conclusion: </strong>13 unique models were identified that evaluated cardiovascular and kidney outcomes in patients with type 2 diabetes. Two models, RECODe and UKPDS-OM2, evaluated all outcomes except for admission to hospital for heart failure. Of all the appraised prognostic models, RECODe had acceptable discrimination and calibration in validation studies for most outcomes; although, additional studies directly comparing models are needed.</p><p><strong>Study registration number: </strong>PROSPERO, CRD42023423075.</p><p><strong>Readers’ note: </strong>This article is a living systematic review that will be updated to reflect emerging evidence. Updates may occur for up to two years from the date of original publication. This version is the original article.</p>\",\"PeriodicalId\":72433,\"journal\":{\"name\":\"BMJ medicine\",\"volume\":\"4 1\",\"pages\":\"e001369\"},\"PeriodicalIF\":10.0000,\"publicationDate\":\"2025-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359462/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjmed-2025-001369\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2025-001369","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Prognostic models for cardiovascular and kidney outcomes in people with type 2 diabetes: living systematic review and meta-analysis of observational studies.
Objective: To summarise available evidence regarding the performance metrics of validated prognostic models on cardiovascular and kidney outcomes in adults with type 2 diabetes mellitus.
Design: Living systematic review and meta-analysis of observational studies.
Data sources: Medline, Embase, Central, and the Cochrane Database of Systematic Reviews from 1 January 2020 to 17 January 2024.
Eligibility criteria for selecting studies: Studies validating prognostic models that predicted all cause and cardiovascular mortality, admission to hospital for heart failure, kidney failure, myocardial infarction, or ischaemic stroke in adults with type 2 diabetes mellitus, including people with established cardiovascular disease or chronic kidney disease, or both. Risk models evaluating composite outcomes were not eligible.
Data synthesis: For each model and outcome, using a random effects model, the reported discrimination measures were pooled, reported as c statistics. Furthermore, when available, calibration plots were reconstructed and interpreted narratively. The Prediction Model Risk of Bias Assessment (PROBAST) tool was used to assess the risk of bias of each analysed study cohort and the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach to evaluate our certainty in the evidence.
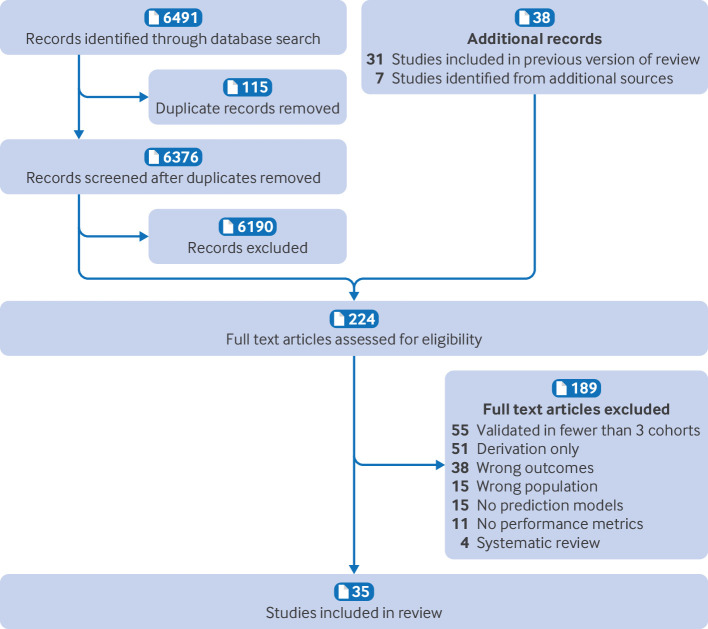
Results: 6529 publications were identified, of which 35 studies reporting on 13 models were included, all of which were developed for general populations with type 2 diabetes but no established cardiovascular disease or chronic kidney disease. Among the identified models, the Risk Equations for Complications of Type 2 Diabetes (RECODe) and the UK Prospective Diabetes Study Outcomes Model 2 (UKPDS-OM2) evaluated all outcomes except for admission to hospital for heart failure. Relative to a threshold c statistic of 0.7, RECODe had an acceptable discrimination for cardiovascular mortality (0.79, high certainty), probably has an acceptable discrimination for myocardial infarction (0.72, moderate certainty) and stroke (0.71, moderate certainty), and may have an acceptable discrimination for kidney failure (0.76, low certainty). High certainty evidence suggests that UKPDS-OM2 has unacceptable discrimination for myocardial infarction (0.64) and stroke (0.65). RECODe showed acceptable calibration for cardiovascular mortality (high certainty), myocardial infarction (high certainty), and kidney failure (moderate certainty) but had unacceptable calibration for stroke (moderate certainty). UKPDS-OM2 showed acceptable calibration for cardiovascular mortality (moderate certainty), stroke (moderate certainty), and kidney failure (low certainty), but may have unacceptable calibration for myocardial infarction (moderate certainty).
Conclusion: 13 unique models were identified that evaluated cardiovascular and kidney outcomes in patients with type 2 diabetes. Two models, RECODe and UKPDS-OM2, evaluated all outcomes except for admission to hospital for heart failure. Of all the appraised prognostic models, RECODe had acceptable discrimination and calibration in validation studies for most outcomes; although, additional studies directly comparing models are needed.
Study registration number: PROSPERO, CRD42023423075.
Readers’ note: This article is a living systematic review that will be updated to reflect emerging evidence. Updates may occur for up to two years from the date of original publication. This version is the original article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


