Philip P Ratnasamy, Sahir S Jabbouri, Gwyneth C Maloy, Arya G Varthi, Daniel R Rubio, Jonathan N Grauer
{"title":"内窥镜腰椎减压术90天内急诊就诊。","authors":"Philip P Ratnasamy, Sahir S Jabbouri, Gwyneth C Maloy, Arya G Varthi, Daniel R Rubio, Jonathan N Grauer","doi":"10.5435/JAAOSGlobal-D-25-00009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background context: </strong>Endoscopic lumbar decompression is growing in popularity as an alternative to an open approach for management of lumbar radiculopathy. Although endoscopic procedures are inherently less invasive, emergency department (ED) visits may occur postoperatively. Although many quality improvement initiatives target readmissions, ED visits may be more common, be a marker of quality of care, affect patient satisfaction, and contribute to healthcare resource utilization and costs.</p><p><strong>Purpose: </strong>To characterize the timing and risk factors of ED utilization following single-level endoscopic lumbar decompression.</p><p><strong>Study design/setting: </strong>Retrospective database review.</p><p><strong>Patient sample: </strong>PearlDiver M165Ortho data set.</p><p><strong>Outcome measures: </strong>Timing of ED utilization following endoscopic lumbar decompression, independent risk factors of ED utilization following endoscopic lumbar decompression, and revision surgery rate among patients who use the ED.</p><p><strong>Methods: </strong>Single-level endoscopic lumbar decompression patients were identified from the PearlDiver M165Ortho data set. Patients were excluded if additional procedures were performed, if they were younger than 18 years, if they had a concomitant diagnosis of trauma, neoplasm, or infection on the day of surgery, or if there was not 90-day follow-up in the data set. Patient factors were extracted, including age, sex, Elixhauser Comorbidity Index, region of the country in which their procedure was performed (Midwest, Northeast, South, West), and patient insurance plan (Commercial, Medicaid, Medicare).The incidence, timing, and frequency of ED utilization within 90 days of endoscopic lumbar decompression was then determined. A baseline rate of weekly ED utilization for the study cohort was calculated based on average weekly ED utilization at 52 to 56 weeks postoperatively. Patient factors predictive of postoperative ED utilization were then determined by univariate and multivariate analyses.</p><p><strong>Results: </strong>Of 1397 endoscopic lumbar decompression patients identified, 151 (10.8%) visited the ED within 90 days of surgery. Of note, approximately 29% of these ED visits occurred in the first 2 postoperative weeks.Multivariate analysis revealed several independent predictors of ED utilization following endoscopic lumbar decompression, including female sex (odds ratio [OR] 1.57 relative to male), higher Elixhauser Comorbidity Index (OR 1.15 per two-point increase), and Medicaid coverage (OR 2.49 relative to Medicare).Of patients who visited the ED, 97 (64.2%) were readmitted. Less than 11 patients who used the ED underwent revision surgery in the subsequent 2 weeks.</p><p><strong>Conclusions: </strong>Following endoscopic lumbar decompression, close to 11% of patients were found to visit the ED in the 90 days following their surgery, most commonly in the first two postoperative weeks. Several factors were independently associated with ED utilization, including female sex, greater comorbidity burden, and having Medicaid insurance. Notably, ED utilization rates following endoscopic lumbar decompression are similar to those following open lumbar decompression previously published in the literature. Thus, patients undergoing endoscopic decompression are at similar risk of postoperative ED utilization-surgeons should be aware of this risk and care pathways should be modified to reduce the occurrence of postoperative ED visits in this population.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 8","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366965/pdf/","citationCount":"0","resultStr":"{\"title\":\"Emergency Department Visits Within Ninety Days of Endoscopic Lumbar Decompression.\",\"authors\":\"Philip P Ratnasamy, Sahir S Jabbouri, Gwyneth C Maloy, Arya G Varthi, Daniel R Rubio, Jonathan N Grauer\",\"doi\":\"10.5435/JAAOSGlobal-D-25-00009\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background context: </strong>Endoscopic lumbar decompression is growing in popularity as an alternative to an open approach for management of lumbar radiculopathy. Although endoscopic procedures are inherently less invasive, emergency department (ED) visits may occur postoperatively. Although many quality improvement initiatives target readmissions, ED visits may be more common, be a marker of quality of care, affect patient satisfaction, and contribute to healthcare resource utilization and costs.</p><p><strong>Purpose: </strong>To characterize the timing and risk factors of ED utilization following single-level endoscopic lumbar decompression.</p><p><strong>Study design/setting: </strong>Retrospective database review.</p><p><strong>Patient sample: </strong>PearlDiver M165Ortho data set.</p><p><strong>Outcome measures: </strong>Timing of ED utilization following endoscopic lumbar decompression, independent risk factors of ED utilization following endoscopic lumbar decompression, and revision surgery rate among patients who use the ED.</p><p><strong>Methods: </strong>Single-level endoscopic lumbar decompression patients were identified from the PearlDiver M165Ortho data set. Patients were excluded if additional procedures were performed, if they were younger than 18 years, if they had a concomitant diagnosis of trauma, neoplasm, or infection on the day of surgery, or if there was not 90-day follow-up in the data set. Patient factors were extracted, including age, sex, Elixhauser Comorbidity Index, region of the country in which their procedure was performed (Midwest, Northeast, South, West), and patient insurance plan (Commercial, Medicaid, Medicare).The incidence, timing, and frequency of ED utilization within 90 days of endoscopic lumbar decompression was then determined. A baseline rate of weekly ED utilization for the study cohort was calculated based on average weekly ED utilization at 52 to 56 weeks postoperatively. Patient factors predictive of postoperative ED utilization were then determined by univariate and multivariate analyses.</p><p><strong>Results: </strong>Of 1397 endoscopic lumbar decompression patients identified, 151 (10.8%) visited the ED within 90 days of surgery. Of note, approximately 29% of these ED visits occurred in the first 2 postoperative weeks.Multivariate analysis revealed several independent predictors of ED utilization following endoscopic lumbar decompression, including female sex (odds ratio [OR] 1.57 relative to male), higher Elixhauser Comorbidity Index (OR 1.15 per two-point increase), and Medicaid coverage (OR 2.49 relative to Medicare).Of patients who visited the ED, 97 (64.2%) were readmitted. Less than 11 patients who used the ED underwent revision surgery in the subsequent 2 weeks.</p><p><strong>Conclusions: </strong>Following endoscopic lumbar decompression, close to 11% of patients were found to visit the ED in the 90 days following their surgery, most commonly in the first two postoperative weeks. Several factors were independently associated with ED utilization, including female sex, greater comorbidity burden, and having Medicaid insurance. Notably, ED utilization rates following endoscopic lumbar decompression are similar to those following open lumbar decompression previously published in the literature. Thus, patients undergoing endoscopic decompression are at similar risk of postoperative ED utilization-surgeons should be aware of this risk and care pathways should be modified to reduce the occurrence of postoperative ED visits in this population.</p>\",\"PeriodicalId\":45062,\"journal\":{\"name\":\"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews\",\"volume\":\"9 8\",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366965/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5435/JAAOSGlobal-D-25-00009\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-25-00009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Emergency Department Visits Within Ninety Days of Endoscopic Lumbar Decompression.
Background context: Endoscopic lumbar decompression is growing in popularity as an alternative to an open approach for management of lumbar radiculopathy. Although endoscopic procedures are inherently less invasive, emergency department (ED) visits may occur postoperatively. Although many quality improvement initiatives target readmissions, ED visits may be more common, be a marker of quality of care, affect patient satisfaction, and contribute to healthcare resource utilization and costs.
Purpose: To characterize the timing and risk factors of ED utilization following single-level endoscopic lumbar decompression.
Study design/setting: Retrospective database review.
Patient sample: PearlDiver M165Ortho data set.
Outcome measures: Timing of ED utilization following endoscopic lumbar decompression, independent risk factors of ED utilization following endoscopic lumbar decompression, and revision surgery rate among patients who use the ED.
Methods: Single-level endoscopic lumbar decompression patients were identified from the PearlDiver M165Ortho data set. Patients were excluded if additional procedures were performed, if they were younger than 18 years, if they had a concomitant diagnosis of trauma, neoplasm, or infection on the day of surgery, or if there was not 90-day follow-up in the data set. Patient factors were extracted, including age, sex, Elixhauser Comorbidity Index, region of the country in which their procedure was performed (Midwest, Northeast, South, West), and patient insurance plan (Commercial, Medicaid, Medicare).The incidence, timing, and frequency of ED utilization within 90 days of endoscopic lumbar decompression was then determined. A baseline rate of weekly ED utilization for the study cohort was calculated based on average weekly ED utilization at 52 to 56 weeks postoperatively. Patient factors predictive of postoperative ED utilization were then determined by univariate and multivariate analyses.
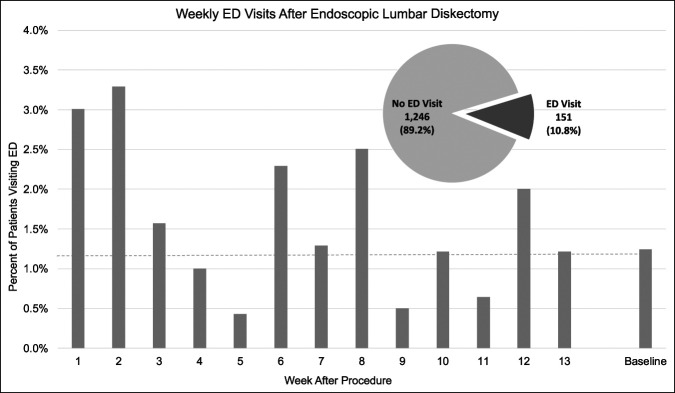
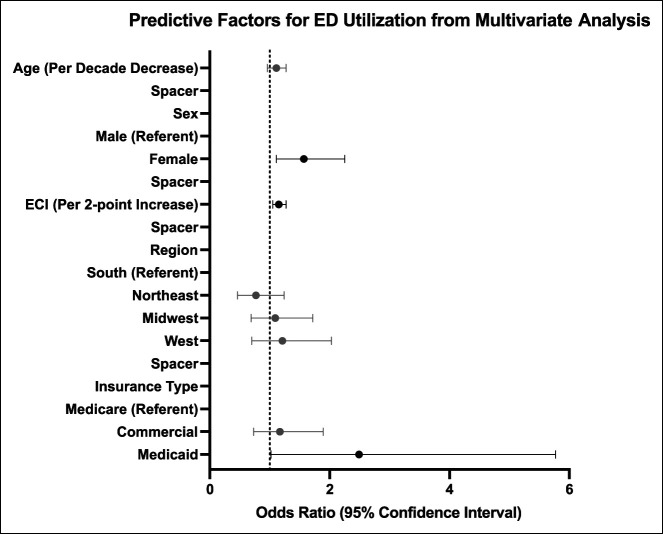
Results: Of 1397 endoscopic lumbar decompression patients identified, 151 (10.8%) visited the ED within 90 days of surgery. Of note, approximately 29% of these ED visits occurred in the first 2 postoperative weeks.Multivariate analysis revealed several independent predictors of ED utilization following endoscopic lumbar decompression, including female sex (odds ratio [OR] 1.57 relative to male), higher Elixhauser Comorbidity Index (OR 1.15 per two-point increase), and Medicaid coverage (OR 2.49 relative to Medicare).Of patients who visited the ED, 97 (64.2%) were readmitted. Less than 11 patients who used the ED underwent revision surgery in the subsequent 2 weeks.
Conclusions: Following endoscopic lumbar decompression, close to 11% of patients were found to visit the ED in the 90 days following their surgery, most commonly in the first two postoperative weeks. Several factors were independently associated with ED utilization, including female sex, greater comorbidity burden, and having Medicaid insurance. Notably, ED utilization rates following endoscopic lumbar decompression are similar to those following open lumbar decompression previously published in the literature. Thus, patients undergoing endoscopic decompression are at similar risk of postoperative ED utilization-surgeons should be aware of this risk and care pathways should be modified to reduce the occurrence of postoperative ED visits in this population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


