Nisarg Radadia, Eldar Priel, Yonni Friedlander, Norman B Konyer, Chynna Huang, Mobin Jamal, Troy Farncombe, Christopher Marriott, Christian Finley, John Agzarian, Michael D Noseworthy, Parameswaran Nair, Yaron Shargall, Sarah Svenningsen
{"title":"通气缺陷负担预测肺癌切除结果","authors":"Nisarg Radadia, Eldar Priel, Yonni Friedlander, Norman B Konyer, Chynna Huang, Mobin Jamal, Troy Farncombe, Christopher Marriott, Christian Finley, John Agzarian, Michael D Noseworthy, Parameswaran Nair, Yaron Shargall, Sarah Svenningsen","doi":"10.1183/23120541.01317-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abnormal ventilation prior to lung cancer resection has not been investigated using modern ventilation imaging modalities and may better predict postoperative outcomes than guideline-recommended lung function tests. Our objective was to quantify the burden of ventilation defects observed using Technegas single-photon emission computed tomography (SPECT) and <sup>129</sup>Xe magnetic resonance imaging (MRI) before lung cancer resection, and to evaluate their association with postoperative pulmonary complications and length of hospital stay.</p><p><strong>Methods: </strong>This was a prospective, 6-week, observational study of adults undergoing lung cancer resection at a single centre. Before lung resection, participants underwent Technegas-SPECT, <sup>129</sup>Xe-MRI, spirometry and measurement of diffusing capacity of the lung for carbon monoxide. Preoperative ventilation defect burden was quantified by the Technegas-SPECT and <sup>129</sup>Xe-MRI ventilation defect percent (VDP). Predictors of complications during the 4-week postoperative period and length of hospital stay were evaluated by logistic and linear regression.</p><p><strong>Results: </strong>Abnormal ventilation was observed preoperatively by Technegas-SPECT and <sup>129</sup>Xe-MRI for 58% (60 of 103) and 73% (74 of 102) of participants, respectively. Preoperative VDPs were higher for participants with postoperative complications compared with those without (SPECT: p=0.01; MRI: p=0.0006) and correlated with length of hospital stay (SPECT: r=0.44, p<0.0001; MRI: r=0.51, p<0.0001). Multivariable models revealed preoperative VDP to be the strongest predictor of postoperative complications (SPECT: OR 1.06, 95% CI 1.01-1.11, p=0.02; MRI: OR 1.11, 95% CI 1.02-1.21, p=0.02) and length of hospital stay (SPECT: β=0.16, p<0.001; MRI: β=0.23, p<0.001).</p><p><strong>Conclusion: </strong>Abnormal ventilation is prevalent prior to lung cancer resection and may be a stronger predictor of postoperative complications and length of hospital stay than standard clinical lung function measures.</p>","PeriodicalId":11739,"journal":{"name":"ERJ Open Research","volume":"11 4","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359065/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ventilation defect burden predicts lung cancer resection outcomes.\",\"authors\":\"Nisarg Radadia, Eldar Priel, Yonni Friedlander, Norman B Konyer, Chynna Huang, Mobin Jamal, Troy Farncombe, Christopher Marriott, Christian Finley, John Agzarian, Michael D Noseworthy, Parameswaran Nair, Yaron Shargall, Sarah Svenningsen\",\"doi\":\"10.1183/23120541.01317-2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Abnormal ventilation prior to lung cancer resection has not been investigated using modern ventilation imaging modalities and may better predict postoperative outcomes than guideline-recommended lung function tests. Our objective was to quantify the burden of ventilation defects observed using Technegas single-photon emission computed tomography (SPECT) and <sup>129</sup>Xe magnetic resonance imaging (MRI) before lung cancer resection, and to evaluate their association with postoperative pulmonary complications and length of hospital stay.</p><p><strong>Methods: </strong>This was a prospective, 6-week, observational study of adults undergoing lung cancer resection at a single centre. Before lung resection, participants underwent Technegas-SPECT, <sup>129</sup>Xe-MRI, spirometry and measurement of diffusing capacity of the lung for carbon monoxide. Preoperative ventilation defect burden was quantified by the Technegas-SPECT and <sup>129</sup>Xe-MRI ventilation defect percent (VDP). Predictors of complications during the 4-week postoperative period and length of hospital stay were evaluated by logistic and linear regression.</p><p><strong>Results: </strong>Abnormal ventilation was observed preoperatively by Technegas-SPECT and <sup>129</sup>Xe-MRI for 58% (60 of 103) and 73% (74 of 102) of participants, respectively. Preoperative VDPs were higher for participants with postoperative complications compared with those without (SPECT: p=0.01; MRI: p=0.0006) and correlated with length of hospital stay (SPECT: r=0.44, p<0.0001; MRI: r=0.51, p<0.0001). Multivariable models revealed preoperative VDP to be the strongest predictor of postoperative complications (SPECT: OR 1.06, 95% CI 1.01-1.11, p=0.02; MRI: OR 1.11, 95% CI 1.02-1.21, p=0.02) and length of hospital stay (SPECT: β=0.16, p<0.001; MRI: β=0.23, p<0.001).</p><p><strong>Conclusion: </strong>Abnormal ventilation is prevalent prior to lung cancer resection and may be a stronger predictor of postoperative complications and length of hospital stay than standard clinical lung function measures.</p>\",\"PeriodicalId\":11739,\"journal\":{\"name\":\"ERJ Open Research\",\"volume\":\"11 4\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359065/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ERJ Open Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1183/23120541.01317-2024\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ERJ Open Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/23120541.01317-2024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Ventilation defect burden predicts lung cancer resection outcomes.
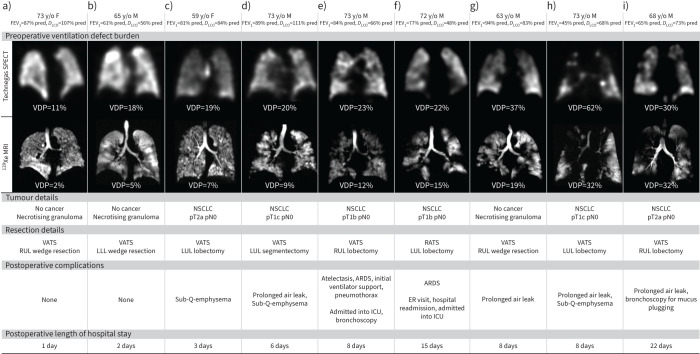
Background: Abnormal ventilation prior to lung cancer resection has not been investigated using modern ventilation imaging modalities and may better predict postoperative outcomes than guideline-recommended lung function tests. Our objective was to quantify the burden of ventilation defects observed using Technegas single-photon emission computed tomography (SPECT) and 129Xe magnetic resonance imaging (MRI) before lung cancer resection, and to evaluate their association with postoperative pulmonary complications and length of hospital stay.
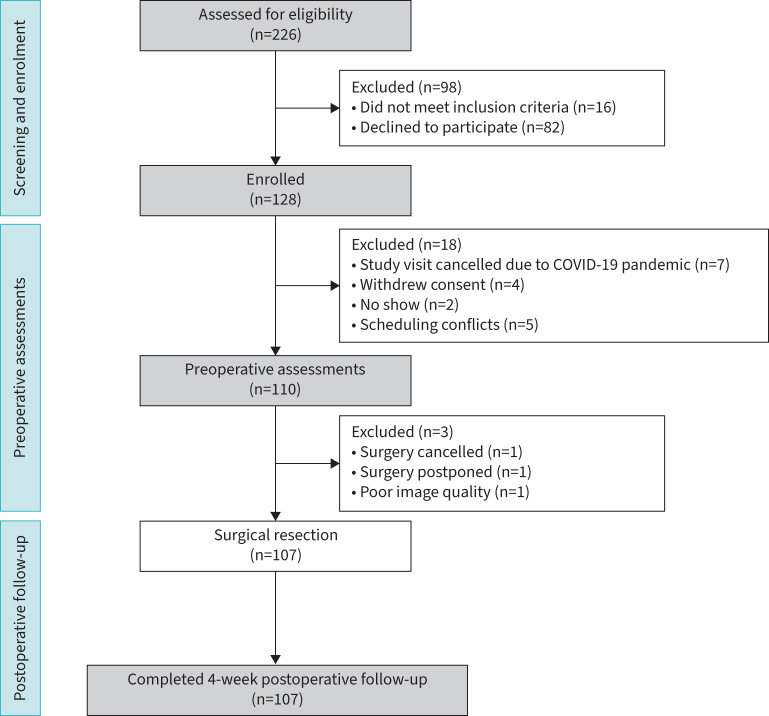
Methods: This was a prospective, 6-week, observational study of adults undergoing lung cancer resection at a single centre. Before lung resection, participants underwent Technegas-SPECT, 129Xe-MRI, spirometry and measurement of diffusing capacity of the lung for carbon monoxide. Preoperative ventilation defect burden was quantified by the Technegas-SPECT and 129Xe-MRI ventilation defect percent (VDP). Predictors of complications during the 4-week postoperative period and length of hospital stay were evaluated by logistic and linear regression.
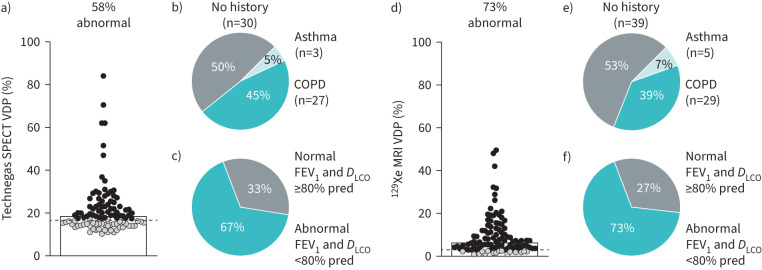
Results: Abnormal ventilation was observed preoperatively by Technegas-SPECT and 129Xe-MRI for 58% (60 of 103) and 73% (74 of 102) of participants, respectively. Preoperative VDPs were higher for participants with postoperative complications compared with those without (SPECT: p=0.01; MRI: p=0.0006) and correlated with length of hospital stay (SPECT: r=0.44, p<0.0001; MRI: r=0.51, p<0.0001). Multivariable models revealed preoperative VDP to be the strongest predictor of postoperative complications (SPECT: OR 1.06, 95% CI 1.01-1.11, p=0.02; MRI: OR 1.11, 95% CI 1.02-1.21, p=0.02) and length of hospital stay (SPECT: β=0.16, p<0.001; MRI: β=0.23, p<0.001).
Conclusion: Abnormal ventilation is prevalent prior to lung cancer resection and may be a stronger predictor of postoperative complications and length of hospital stay than standard clinical lung function measures.
期刊介绍:
ERJ Open Research is a fully open access original research journal, published online by the European Respiratory Society. The journal aims to publish high-quality work in all fields of respiratory science and medicine, covering basic science, clinical translational science and clinical medicine. The journal was created to help fulfil the ERS objective to disseminate scientific and educational material to its members and to the medical community, but also to provide researchers with an affordable open access specialty journal in which to publish their work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


