Keith Bodger, William Tench, Thomas Mair, Pieta Schofield, Susanna Dodd, Benjamin Silberberg, Kate M Fleming, Steve Hood
{"title":"在英国,酒精相关性肝病周末急诊入院与30天死亡率增加相关:一项使用临床实践研究数据链的记录关联研究","authors":"Keith Bodger, William Tench, Thomas Mair, Pieta Schofield, Susanna Dodd, Benjamin Silberberg, Kate M Fleming, Steve Hood","doi":"10.1136/bmjgast-2025-001831","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Deficiencies have been highlighted in acute hospital care for alcohol-related liver disease (ARLD). Such problems may be worse at weekends (WEs). Increased 30-day mortality for WE admissions has been reported for several acute conditions, but data for ARLD are limited. We aimed to compare patient and pathway characteristics between WE and weekday (WD) admissions and investigate the 'weekend effect' on mortality.</p><p><strong>Methods: </strong>Retrospective cohort study (2008-2018) using linked electronic databases (Hospital Episode Statistics-Clinical Practice Research Datalink and death registration) including 17 575 first emergency admissions identified using the Liverpool ARLD algorithm.</p><p><strong>Exposure: </strong>WE admission (Saturday or Sunday).</p><p><strong>Main outcome: </strong>all-cause death within 30 days. Covariates included socio-demographic characteristics, pathway characteristics (pre-admission contacts and admission method) and markers of severity (recorded stage of liver disease, ascites and varices, comorbidity). Alternative risk-adjustment methods were used, including standard regression and propensity-weighted analysis (Inverse Probability of Treatment Weighting).</p><p><strong>Results: </strong>3249 admissions (18.5%) were at WE. Unadjusted 30-day mortality was significantly higher for WE versus WD (17.1% vs 15.5%, p=0.018). All models demonstrated increased odds of death for WE admissions with adjusted ORs ranging from 1.15 to 1.23 (relative risk of 1.12-1.19). Causes of death did not vary by admission day and effect was consistent across subgroups. Findings were robust to sensitivity analyses restricting the cohort to patients admitted directly from Accident and Emergency department (A&E), or cirrhosis or ascites but not varices.</p><p><strong>Conclusion: </strong>First ARLD admissions at the WE experienced a 12-19% increase in 30-day mortality risk compared with WD. Although residual confounding cannot be excluded, this suggests the possibility of avoidable mortality among those hospitalised at WEs. Services should be alert to risks of WE effects when planning care.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":"12 1","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366567/pdf/","citationCount":"0","resultStr":"{\"title\":\"Increased 30-day mortality associated with weekend emergency admission for alcohol-related liver disease in England: a record-linkage study using the Clinical Practice Research Datalink.\",\"authors\":\"Keith Bodger, William Tench, Thomas Mair, Pieta Schofield, Susanna Dodd, Benjamin Silberberg, Kate M Fleming, Steve Hood\",\"doi\":\"10.1136/bmjgast-2025-001831\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Deficiencies have been highlighted in acute hospital care for alcohol-related liver disease (ARLD). Such problems may be worse at weekends (WEs). Increased 30-day mortality for WE admissions has been reported for several acute conditions, but data for ARLD are limited. We aimed to compare patient and pathway characteristics between WE and weekday (WD) admissions and investigate the 'weekend effect' on mortality.</p><p><strong>Methods: </strong>Retrospective cohort study (2008-2018) using linked electronic databases (Hospital Episode Statistics-Clinical Practice Research Datalink and death registration) including 17 575 first emergency admissions identified using the Liverpool ARLD algorithm.</p><p><strong>Exposure: </strong>WE admission (Saturday or Sunday).</p><p><strong>Main outcome: </strong>all-cause death within 30 days. Covariates included socio-demographic characteristics, pathway characteristics (pre-admission contacts and admission method) and markers of severity (recorded stage of liver disease, ascites and varices, comorbidity). Alternative risk-adjustment methods were used, including standard regression and propensity-weighted analysis (Inverse Probability of Treatment Weighting).</p><p><strong>Results: </strong>3249 admissions (18.5%) were at WE. Unadjusted 30-day mortality was significantly higher for WE versus WD (17.1% vs 15.5%, p=0.018). All models demonstrated increased odds of death for WE admissions with adjusted ORs ranging from 1.15 to 1.23 (relative risk of 1.12-1.19). Causes of death did not vary by admission day and effect was consistent across subgroups. Findings were robust to sensitivity analyses restricting the cohort to patients admitted directly from Accident and Emergency department (A&E), or cirrhosis or ascites but not varices.</p><p><strong>Conclusion: </strong>First ARLD admissions at the WE experienced a 12-19% increase in 30-day mortality risk compared with WD. Although residual confounding cannot be excluded, this suggests the possibility of avoidable mortality among those hospitalised at WEs. Services should be alert to risks of WE effects when planning care.</p>\",\"PeriodicalId\":9235,\"journal\":{\"name\":\"BMJ Open Gastroenterology\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366567/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjgast-2025-001831\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjgast-2025-001831","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:酒精相关性肝病(ARLD)的急性医院护理的不足之处已被强调。这样的问题在周末可能会更严重。据报道,在一些急性病中,WE入院的30天死亡率增加,但ARLD的数据有限。我们的目的是比较工作日入院和工作日入院的患者和通路特征,并调查“周末效应”对死亡率的影响。方法:回顾性队列研究(2008-2018),使用链接电子数据库(医院事件统计-临床实践研究数据链和死亡登记),包括使用利物浦ARLD算法确定的17575例首次急诊患者。曝光:WE入场(周六或周日)。主要结局:30天内全因死亡。协变量包括社会人口学特征、途径特征(入院前接触者和入院方法)和严重程度标记(肝脏疾病、腹水和静脉曲张、合并症的记录分期)。采用替代风险调整方法,包括标准回归和倾向加权分析(处理加权逆概率)。结果:3249例(18.5%)入院。未调整的30天死亡率WE明显高于WD (17.1% vs 15.5%, p=0.018)。所有模型均显示WE入院患者的死亡几率增加,调整后的or范围为1.15至1.23(相对风险为1.12-1.19)。死亡原因没有随入院日期的变化而变化,亚组间的效果是一致的。敏感性分析将研究对象限制为直接从急诊科(A&E)入院的患者,或肝硬化或腹水但不包括静脉曲张的患者,结果是可靠的。结论:与WD相比,WE的首次ARLD入院患者30天死亡风险增加了12-19%。虽然不能排除残留的混杂因素,但这表明在WEs住院的患者中可能存在可避免的死亡率。服务部门在规划护理时应警惕WE效应的风险。
Increased 30-day mortality associated with weekend emergency admission for alcohol-related liver disease in England: a record-linkage study using the Clinical Practice Research Datalink.
Objective: Deficiencies have been highlighted in acute hospital care for alcohol-related liver disease (ARLD). Such problems may be worse at weekends (WEs). Increased 30-day mortality for WE admissions has been reported for several acute conditions, but data for ARLD are limited. We aimed to compare patient and pathway characteristics between WE and weekday (WD) admissions and investigate the 'weekend effect' on mortality.
Methods: Retrospective cohort study (2008-2018) using linked electronic databases (Hospital Episode Statistics-Clinical Practice Research Datalink and death registration) including 17 575 first emergency admissions identified using the Liverpool ARLD algorithm.
Exposure: WE admission (Saturday or Sunday).
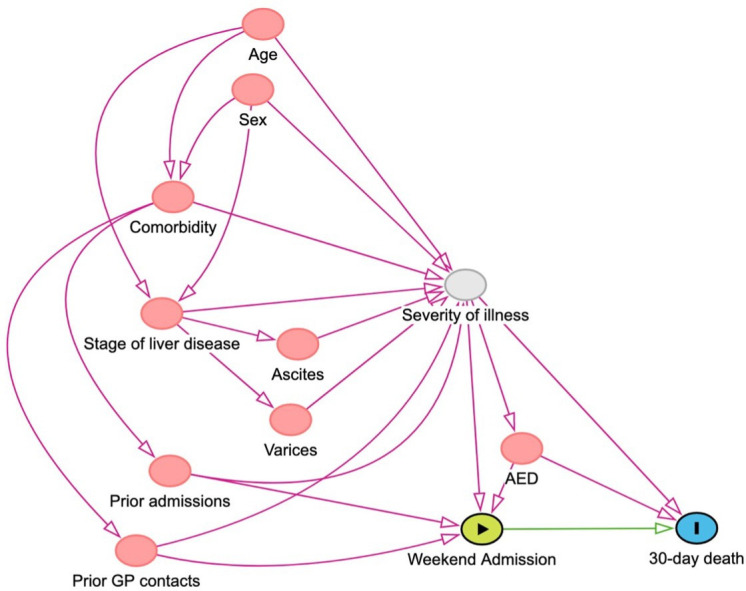
Main outcome: all-cause death within 30 days. Covariates included socio-demographic characteristics, pathway characteristics (pre-admission contacts and admission method) and markers of severity (recorded stage of liver disease, ascites and varices, comorbidity). Alternative risk-adjustment methods were used, including standard regression and propensity-weighted analysis (Inverse Probability of Treatment Weighting).
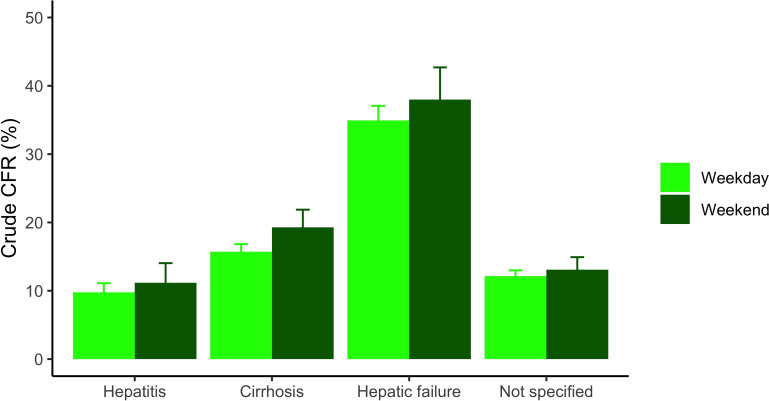
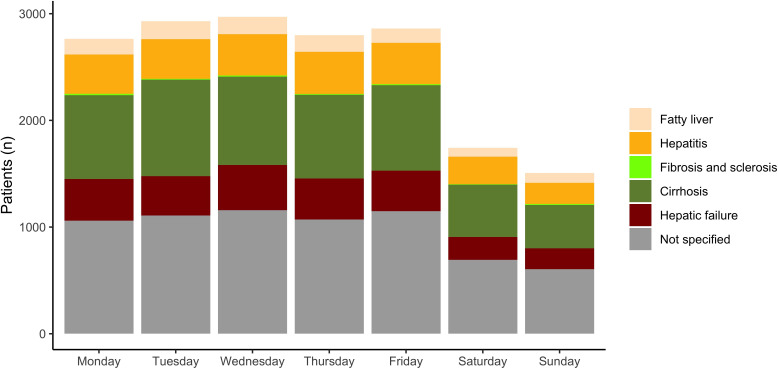
Results: 3249 admissions (18.5%) were at WE. Unadjusted 30-day mortality was significantly higher for WE versus WD (17.1% vs 15.5%, p=0.018). All models demonstrated increased odds of death for WE admissions with adjusted ORs ranging from 1.15 to 1.23 (relative risk of 1.12-1.19). Causes of death did not vary by admission day and effect was consistent across subgroups. Findings were robust to sensitivity analyses restricting the cohort to patients admitted directly from Accident and Emergency department (A&E), or cirrhosis or ascites but not varices.
Conclusion: First ARLD admissions at the WE experienced a 12-19% increase in 30-day mortality risk compared with WD. Although residual confounding cannot be excluded, this suggests the possibility of avoidable mortality among those hospitalised at WEs. Services should be alert to risks of WE effects when planning care.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


