Meng-Yu Wu, Giou-Teng Yiang, Sy-Jou Chen, Hon-Ping Ma, Mau-Roung Lin
{"title":"现场时间和院前干预对创伤患者住院死亡率的影响。","authors":"Meng-Yu Wu, Giou-Teng Yiang, Sy-Jou Chen, Hon-Ping Ma, Mau-Roung Lin","doi":"10.1186/s12873-025-01324-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to investigate the impact of the type and number of prehospital interventions, in addition to prehospital time intervals, on inhospital mortality among trauma patients.</p><p><strong>Methods: </strong>According to a 13-year prospective trauma registry, three prehospital time intervals of response time, on-scene time, and transport time were assessed. Prehospital interventions were classified into four categories: stop bleeding strategies, immobilization, basic airway management, and advanced resuscitation.</p><p><strong>Results: </strong>A total of 13,533 patients were included. Relative to patients not receiving prehospital interventions, there was longer on-scene time for those who received immobilization (10.4 vs. 8.68 min), basic airway management (11.4 vs. 9.40 min), and advanced resuscitation (12.6 vs. 9.53 min). Furthermore, relative to patients who survived in hospital, those who died significantly had longer on-scene time (11.4 vs. 9.64 min) and sustained immobilization (74.7% vs. 52.5%), basic airway management (30.7% vs. 7.6%), advanced resuscitation (32.0% vs. 0.1%), and ≥ 4 prehospital interventions (30.4% vs. 4.6%). Results of the multivariable logistic regression analysis shows that without adjustment for type and number of prehospital interventions, longer on-scene time (odds ratio [OR] = 1.03; 95% confidence interval [CI], 1.01-1.04) were significantly associated with increased mortality; however, after additional adjustment for type and number of prehospital interventions, no significant association between each of the three prehospital time intervals and mortality was detected. Furthermore, compared to patients who did not receive prehospital interventions, those who received wound packing/compression had a significantly lower risk of mortality (OR = 0.54; 95% CI, 0.36-0.80), whereas those who received basic airway management (OR = 1.73; 95% CI, 1.15-2.60), advanced resuscitation (OR = 33.4; 95% CI, 14.9-75.0), and three (OR = 2.60; 95% CI, 1.01-6.93) and ≥ 4 (OR = 2.97; 95% CI, 1.01-9.63) prehospital interventions had a significantly higher risk of mortality.</p><p><strong>Conclusions: </strong>There exists a tradeoff between prehospital trauma interventions and shortening on-scene time for mortality risk; however, implementing some interventions for hemorrhage control and hemostatic resuscitation can benefit the survival of trauma patients the most.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"163"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366050/pdf/","citationCount":"0","resultStr":"{\"title\":\"Influence of on-scene time and prehospital interventions on inhospital mortality in trauma patients.\",\"authors\":\"Meng-Yu Wu, Giou-Teng Yiang, Sy-Jou Chen, Hon-Ping Ma, Mau-Roung Lin\",\"doi\":\"10.1186/s12873-025-01324-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aimed to investigate the impact of the type and number of prehospital interventions, in addition to prehospital time intervals, on inhospital mortality among trauma patients.</p><p><strong>Methods: </strong>According to a 13-year prospective trauma registry, three prehospital time intervals of response time, on-scene time, and transport time were assessed. Prehospital interventions were classified into four categories: stop bleeding strategies, immobilization, basic airway management, and advanced resuscitation.</p><p><strong>Results: </strong>A total of 13,533 patients were included. Relative to patients not receiving prehospital interventions, there was longer on-scene time for those who received immobilization (10.4 vs. 8.68 min), basic airway management (11.4 vs. 9.40 min), and advanced resuscitation (12.6 vs. 9.53 min). Furthermore, relative to patients who survived in hospital, those who died significantly had longer on-scene time (11.4 vs. 9.64 min) and sustained immobilization (74.7% vs. 52.5%), basic airway management (30.7% vs. 7.6%), advanced resuscitation (32.0% vs. 0.1%), and ≥ 4 prehospital interventions (30.4% vs. 4.6%). Results of the multivariable logistic regression analysis shows that without adjustment for type and number of prehospital interventions, longer on-scene time (odds ratio [OR] = 1.03; 95% confidence interval [CI], 1.01-1.04) were significantly associated with increased mortality; however, after additional adjustment for type and number of prehospital interventions, no significant association between each of the three prehospital time intervals and mortality was detected. Furthermore, compared to patients who did not receive prehospital interventions, those who received wound packing/compression had a significantly lower risk of mortality (OR = 0.54; 95% CI, 0.36-0.80), whereas those who received basic airway management (OR = 1.73; 95% CI, 1.15-2.60), advanced resuscitation (OR = 33.4; 95% CI, 14.9-75.0), and three (OR = 2.60; 95% CI, 1.01-6.93) and ≥ 4 (OR = 2.97; 95% CI, 1.01-9.63) prehospital interventions had a significantly higher risk of mortality.</p><p><strong>Conclusions: </strong>There exists a tradeoff between prehospital trauma interventions and shortening on-scene time for mortality risk; however, implementing some interventions for hemorrhage control and hemostatic resuscitation can benefit the survival of trauma patients the most.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"25 1\",\"pages\":\"163\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366050/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-025-01324-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01324-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究旨在探讨院前干预的类型和次数以及院前时间间隔对创伤患者住院死亡率的影响。方法:根据13年的前瞻性创伤登记,评估三个院前时间间隔的反应时间、现场时间和运输时间。院前干预分为四类:止血策略、固定、基本气道管理和高级复苏。结果:共纳入13533例患者。与未接受院前干预的患者相比,接受固定(10.4 vs. 8.68 min)、基础气道管理(11.4 vs. 9.40 min)和高级复苏(12.6 vs. 9.53 min)的患者在现场的时间更长。此外,与在医院存活的患者相比,死亡患者的现场时间更长(11.4分钟vs. 9.64分钟),持续固定(74.7% vs. 52.5%),基本气道管理(30.7% vs. 7.6%),高级复苏(32.0% vs. 0.1%),院前干预≥4次(30.4% vs. 4.6%)。多变量logistic回归分析结果显示,在不调整院前干预类型和次数的情况下,较长的现场时间(优势比[OR] = 1.03; 95%可信区间[CI], 1.01-1.04)与死亡率增加显著相关;然而,在对院前干预的类型和数量进行额外调整后,没有发现三种院前时间间隔与死亡率之间的显著关联。此外,与未接受院前干预的患者相比,接受伤口填塞/压缩的患者死亡风险显著降低(OR = 0.54, 95% CI, 0.36-0.80),而接受基本气道管理(OR = 1.73, 95% CI, 1.15-2.60)、高级复苏(OR = 33.4, 95% CI, 14.9-75.0)、3次(OR = 2.60, 95% CI, 1.01-6.93)和≥4次(OR = 2.97, 95% CI, 1.01-9.63)院前干预的患者死亡风险显著升高。结论:院前创伤干预与缩短现场死亡时间之间存在权衡;然而,实施一些控制出血和止血复苏的干预措施对创伤患者的生存最为有利。临床试验号:不适用。
Influence of on-scene time and prehospital interventions on inhospital mortality in trauma patients.
Objective: This study aimed to investigate the impact of the type and number of prehospital interventions, in addition to prehospital time intervals, on inhospital mortality among trauma patients.
Methods: According to a 13-year prospective trauma registry, three prehospital time intervals of response time, on-scene time, and transport time were assessed. Prehospital interventions were classified into four categories: stop bleeding strategies, immobilization, basic airway management, and advanced resuscitation.
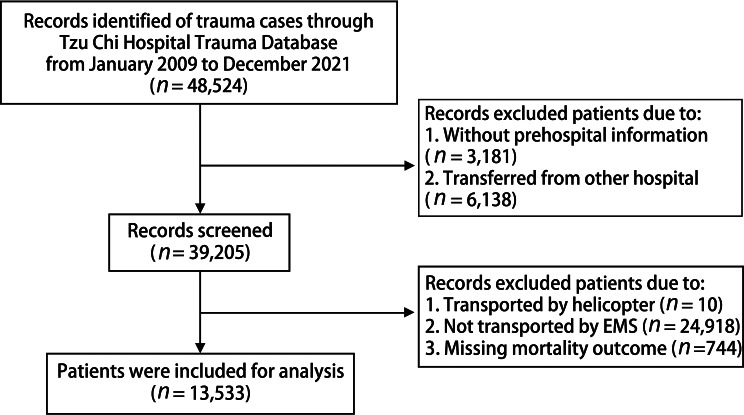
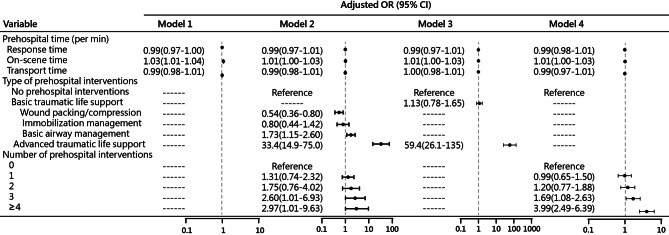
Results: A total of 13,533 patients were included. Relative to patients not receiving prehospital interventions, there was longer on-scene time for those who received immobilization (10.4 vs. 8.68 min), basic airway management (11.4 vs. 9.40 min), and advanced resuscitation (12.6 vs. 9.53 min). Furthermore, relative to patients who survived in hospital, those who died significantly had longer on-scene time (11.4 vs. 9.64 min) and sustained immobilization (74.7% vs. 52.5%), basic airway management (30.7% vs. 7.6%), advanced resuscitation (32.0% vs. 0.1%), and ≥ 4 prehospital interventions (30.4% vs. 4.6%). Results of the multivariable logistic regression analysis shows that without adjustment for type and number of prehospital interventions, longer on-scene time (odds ratio [OR] = 1.03; 95% confidence interval [CI], 1.01-1.04) were significantly associated with increased mortality; however, after additional adjustment for type and number of prehospital interventions, no significant association between each of the three prehospital time intervals and mortality was detected. Furthermore, compared to patients who did not receive prehospital interventions, those who received wound packing/compression had a significantly lower risk of mortality (OR = 0.54; 95% CI, 0.36-0.80), whereas those who received basic airway management (OR = 1.73; 95% CI, 1.15-2.60), advanced resuscitation (OR = 33.4; 95% CI, 14.9-75.0), and three (OR = 2.60; 95% CI, 1.01-6.93) and ≥ 4 (OR = 2.97; 95% CI, 1.01-9.63) prehospital interventions had a significantly higher risk of mortality.
Conclusions: There exists a tradeoff between prehospital trauma interventions and shortening on-scene time for mortality risk; however, implementing some interventions for hemorrhage control and hemostatic resuscitation can benefit the survival of trauma patients the most.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


