Junichi Ishigami, Aditya Surapaneni, Kunihiro Matsushita, Josef Coresh, Morgan E Grams, Shoshana H Ballew, Yingying Sang, Benedicte Stengel, Johan Ärnlöv, Samira Bell, Juan-Jesus Carrero, Alexander R Chang, Elizabeth L Ciemins, Richard Haynes, Joachim Ix, Fruzsina Kotsis, Jennifer S Lees, Krutika Pandit, Panduranga Rao, Cassianne Robinson-Cohen, Natalia Alencar de Pinho, Keiichi Sumida
{"title":"估计肾小球滤过率、蛋白尿和感染风险:个体参与者数据的协作荟萃分析。","authors":"Junichi Ishigami, Aditya Surapaneni, Kunihiro Matsushita, Josef Coresh, Morgan E Grams, Shoshana H Ballew, Yingying Sang, Benedicte Stengel, Johan Ärnlöv, Samira Bell, Juan-Jesus Carrero, Alexander R Chang, Elizabeth L Ciemins, Richard Haynes, Joachim Ix, Fruzsina Kotsis, Jennifer S Lees, Krutika Pandit, Panduranga Rao, Cassianne Robinson-Cohen, Natalia Alencar de Pinho, Keiichi Sumida","doi":"10.1016/j.eclinm.2025.103372","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infections are a major cause of hospitalization in people with chronic kidney disease (CKD), with incidence similar to cardiovascular disease, yet the risk of infection has not been systematically studied across stages of CKD.</p><p><strong>Methods: </strong>We conducted a meta-analysis of individual participant data including 1,246,912 individuals across 47 cohorts in the CKD Prognosis Consortium, with information on estimated glomerular filtration rate based on serum creatinine (eGFRcr) and urinary albuminuria (ACR) (or proteinuria converted to ACR), to examine the association of eGFR and ACR with the risk of hospitalization with infection. Outcomes were ascertained through diagnostic codes on hospital discharge records relevant to acute infections (i.e., upper and lower respiratory tract, urinary tract, skin and soft tissue, musculoskeletal, gastrointestinal tract, genital, nervous system, and cardiovascular system infections, and sepsis). Follow-up was censored on December 31, 2019 or on the last date of cohort follow-up, whichever was earlier. Multivariable Cox models were used to estimate hazard ratios (HRs).</p><p><strong>Findings: </strong>During follow-up, 170,864 (13.7%) individuals had a hospitalization with infection (IR, 22.0 [IQI, 16.2-31.0] per 1000 person-yrs). In Cox models, compared to eGFRcr 90-104 ml/min/1.73 m<sup>2</sup> and ACR <10 mg/g, lower eGFRcr and higher ACR were each independently associated with an increased hazard of infection in a graded manner, including in eGFRcr 60-89 and 45-59 ml/min/1.73 m<sup>2</sup> (adjusted HRs [95% CI], 1.09 [1.06-1.13] and 1.39 [1.34-1.45]) and ACR 10-29 and 30-299 mg/g (1.40 [1.33-1.47] and 1.82 [1.72-1.92]). High eGFRcr ≥105 ml/min/1.73 m<sup>2</sup> was also associated with the risk of infection (1.22 [1.17-1.26]). Combined, eGFRcr <30 ml/min/1.73 m<sup>2</sup> and ACR ≥ 300 mg/g were associated with more than 6-fold higher hazard of infections (6.27 [5.70-6.90]). These findings were consistent across infection subtypes (e.g., HRs for lower respiratory tract infections, 1.26 [1.22-1.30] per -15 ml/min/1.73 m<sup>2</sup> in eGFR and 1.48 [1.44-1.53] per 8-fold increase in ACR).</p><p><strong>Interpretation: </strong>Lower kidney function and higher albuminuria were independently associated with higher risk of infection. The risk was elevated even in mild to moderate CKD, with the highest risk seen in the most advanced stage of CKD. Infection prevention measures should target individuals across all CKD stages.</p><p><strong>Funding: </strong>US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases.</p>","PeriodicalId":11393,"journal":{"name":"EClinicalMedicine","volume":"86 ","pages":"103372"},"PeriodicalIF":10.0000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12337016/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimated glomerular filtration rate, albuminuria, and risk of infection: a collaborative meta-analysis of individual participant data.\",\"authors\":\"Junichi Ishigami, Aditya Surapaneni, Kunihiro Matsushita, Josef Coresh, Morgan E Grams, Shoshana H Ballew, Yingying Sang, Benedicte Stengel, Johan Ärnlöv, Samira Bell, Juan-Jesus Carrero, Alexander R Chang, Elizabeth L Ciemins, Richard Haynes, Joachim Ix, Fruzsina Kotsis, Jennifer S Lees, Krutika Pandit, Panduranga Rao, Cassianne Robinson-Cohen, Natalia Alencar de Pinho, Keiichi Sumida\",\"doi\":\"10.1016/j.eclinm.2025.103372\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Infections are a major cause of hospitalization in people with chronic kidney disease (CKD), with incidence similar to cardiovascular disease, yet the risk of infection has not been systematically studied across stages of CKD.</p><p><strong>Methods: </strong>We conducted a meta-analysis of individual participant data including 1,246,912 individuals across 47 cohorts in the CKD Prognosis Consortium, with information on estimated glomerular filtration rate based on serum creatinine (eGFRcr) and urinary albuminuria (ACR) (or proteinuria converted to ACR), to examine the association of eGFR and ACR with the risk of hospitalization with infection. Outcomes were ascertained through diagnostic codes on hospital discharge records relevant to acute infections (i.e., upper and lower respiratory tract, urinary tract, skin and soft tissue, musculoskeletal, gastrointestinal tract, genital, nervous system, and cardiovascular system infections, and sepsis). Follow-up was censored on December 31, 2019 or on the last date of cohort follow-up, whichever was earlier. Multivariable Cox models were used to estimate hazard ratios (HRs).</p><p><strong>Findings: </strong>During follow-up, 170,864 (13.7%) individuals had a hospitalization with infection (IR, 22.0 [IQI, 16.2-31.0] per 1000 person-yrs). In Cox models, compared to eGFRcr 90-104 ml/min/1.73 m<sup>2</sup> and ACR <10 mg/g, lower eGFRcr and higher ACR were each independently associated with an increased hazard of infection in a graded manner, including in eGFRcr 60-89 and 45-59 ml/min/1.73 m<sup>2</sup> (adjusted HRs [95% CI], 1.09 [1.06-1.13] and 1.39 [1.34-1.45]) and ACR 10-29 and 30-299 mg/g (1.40 [1.33-1.47] and 1.82 [1.72-1.92]). High eGFRcr ≥105 ml/min/1.73 m<sup>2</sup> was also associated with the risk of infection (1.22 [1.17-1.26]). Combined, eGFRcr <30 ml/min/1.73 m<sup>2</sup> and ACR ≥ 300 mg/g were associated with more than 6-fold higher hazard of infections (6.27 [5.70-6.90]). These findings were consistent across infection subtypes (e.g., HRs for lower respiratory tract infections, 1.26 [1.22-1.30] per -15 ml/min/1.73 m<sup>2</sup> in eGFR and 1.48 [1.44-1.53] per 8-fold increase in ACR).</p><p><strong>Interpretation: </strong>Lower kidney function and higher albuminuria were independently associated with higher risk of infection. The risk was elevated even in mild to moderate CKD, with the highest risk seen in the most advanced stage of CKD. Infection prevention measures should target individuals across all CKD stages.</p><p><strong>Funding: </strong>US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases.</p>\",\"PeriodicalId\":11393,\"journal\":{\"name\":\"EClinicalMedicine\",\"volume\":\"86 \",\"pages\":\"103372\"},\"PeriodicalIF\":10.0000,\"publicationDate\":\"2025-07-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12337016/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"EClinicalMedicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.eclinm.2025.103372\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"EClinicalMedicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.eclinm.2025.103372","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Estimated glomerular filtration rate, albuminuria, and risk of infection: a collaborative meta-analysis of individual participant data.
Background: Infections are a major cause of hospitalization in people with chronic kidney disease (CKD), with incidence similar to cardiovascular disease, yet the risk of infection has not been systematically studied across stages of CKD.
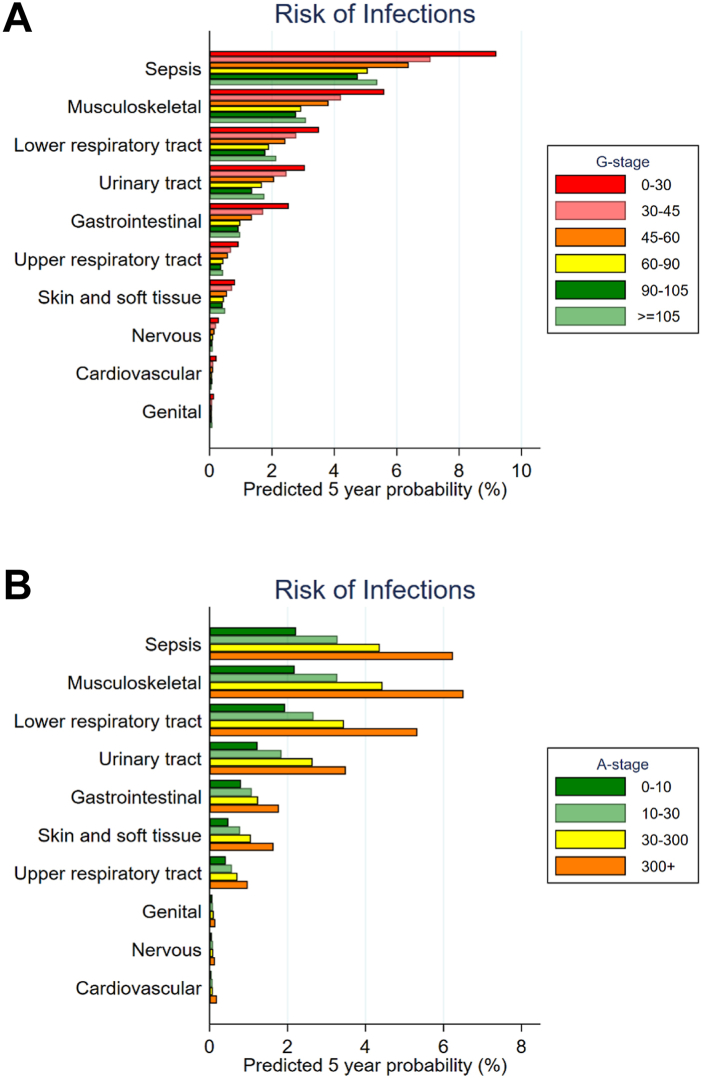
Methods: We conducted a meta-analysis of individual participant data including 1,246,912 individuals across 47 cohorts in the CKD Prognosis Consortium, with information on estimated glomerular filtration rate based on serum creatinine (eGFRcr) and urinary albuminuria (ACR) (or proteinuria converted to ACR), to examine the association of eGFR and ACR with the risk of hospitalization with infection. Outcomes were ascertained through diagnostic codes on hospital discharge records relevant to acute infections (i.e., upper and lower respiratory tract, urinary tract, skin and soft tissue, musculoskeletal, gastrointestinal tract, genital, nervous system, and cardiovascular system infections, and sepsis). Follow-up was censored on December 31, 2019 or on the last date of cohort follow-up, whichever was earlier. Multivariable Cox models were used to estimate hazard ratios (HRs).
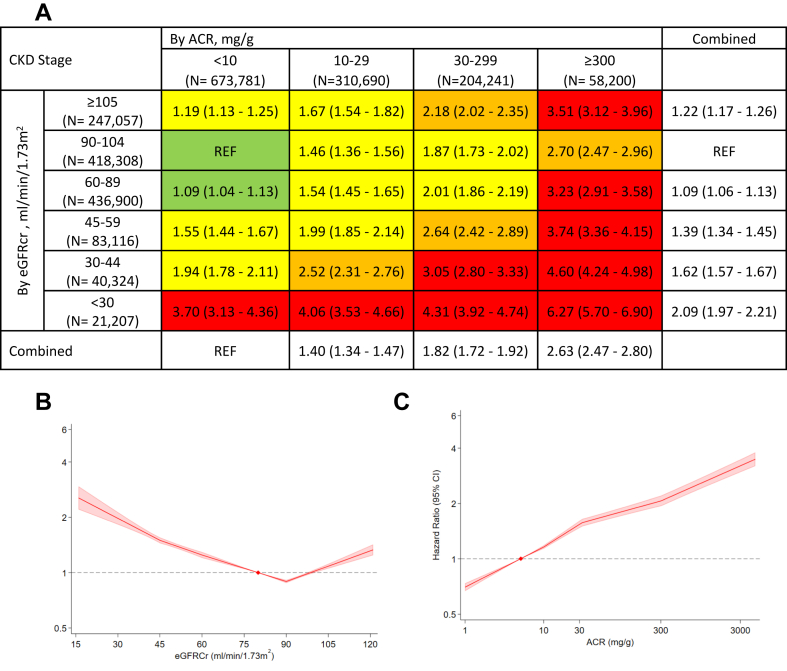
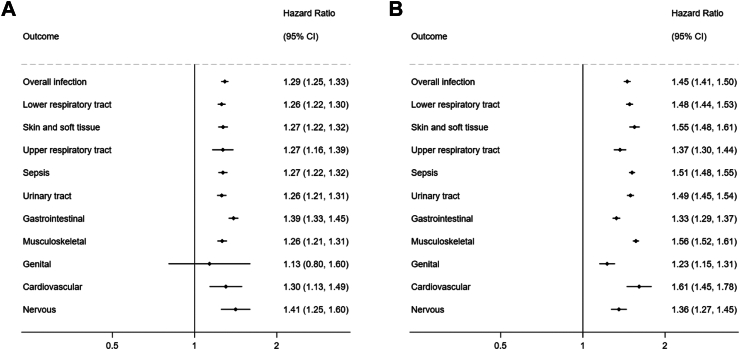
Findings: During follow-up, 170,864 (13.7%) individuals had a hospitalization with infection (IR, 22.0 [IQI, 16.2-31.0] per 1000 person-yrs). In Cox models, compared to eGFRcr 90-104 ml/min/1.73 m2 and ACR <10 mg/g, lower eGFRcr and higher ACR were each independently associated with an increased hazard of infection in a graded manner, including in eGFRcr 60-89 and 45-59 ml/min/1.73 m2 (adjusted HRs [95% CI], 1.09 [1.06-1.13] and 1.39 [1.34-1.45]) and ACR 10-29 and 30-299 mg/g (1.40 [1.33-1.47] and 1.82 [1.72-1.92]). High eGFRcr ≥105 ml/min/1.73 m2 was also associated with the risk of infection (1.22 [1.17-1.26]). Combined, eGFRcr <30 ml/min/1.73 m2 and ACR ≥ 300 mg/g were associated with more than 6-fold higher hazard of infections (6.27 [5.70-6.90]). These findings were consistent across infection subtypes (e.g., HRs for lower respiratory tract infections, 1.26 [1.22-1.30] per -15 ml/min/1.73 m2 in eGFR and 1.48 [1.44-1.53] per 8-fold increase in ACR).
Interpretation: Lower kidney function and higher albuminuria were independently associated with higher risk of infection. The risk was elevated even in mild to moderate CKD, with the highest risk seen in the most advanced stage of CKD. Infection prevention measures should target individuals across all CKD stages.
Funding: US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases.
期刊介绍:
eClinicalMedicine is a gold open-access clinical journal designed to support frontline health professionals in addressing the complex and rapid health transitions affecting societies globally. The journal aims to assist practitioners in overcoming healthcare challenges across diverse communities, spanning diagnosis, treatment, prevention, and health promotion. Integrating disciplines from various specialties and life stages, it seeks to enhance health systems as fundamental institutions within societies. With a forward-thinking approach, eClinicalMedicine aims to redefine the future of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


