Shinichiro Yoshida, Akira Babazono, Ning Liu, Reiko Yamao, Reiko Ishihara
{"title":"老年感染性休克患者的地区差异和死亡相关危险因素:多水平Logistic回归模型的管理数据分析。","authors":"Shinichiro Yoshida, Akira Babazono, Ning Liu, Reiko Yamao, Reiko Ishihara","doi":"10.31662/jmaj.2024-0331","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Variations in intensive care unit (ICU) policies and physician characteristics influence mortality, potentially leading to regional differences in mortality rates. Previous studies have not specifically focused on septic shock or older patients and have lacked consideration of the context effect. We hypothesized that regional variability in mortality exists among older patients with septic shock and investigated factors associated with mortality.</p><p><strong>Methods: </strong>Administrative medical claims data were analyzed. Participants were enrolled from April 2015 to March 2020 in Fukuoka Prefecture, Japan. ICU physicians were classified based on board certification in intensive care medicine as either \"intensivists\" or \"ICU-dedicated physicians\". The primary outcome was 28-day mortality after ICU admission. Data from all ICUs in Fukuoka Prefecture and 9 secondary medical areas were analyzed. We calculated and compared the 28-day mortality rates across regions. Multilevel logistic regression analyses were conducted to adjust for the context effect.</p><p><strong>Results: </strong>Among the 1,238 participants, mortality across regions ranged from 18.3% to 41.4%. Based on multilevel logistic analyses, age, sex, postsurgical admission, and the number of ICU beds per intensivist were significantly associated with mortality. The adjusted odds ratio from the multilevel analysis for having no intensivists versus having ≥1 intensivist per 4 ICU beds was 1.99 (95% confidence interval 1.15-3.44, p = 0.01).</p><p><strong>Conclusions: </strong>After accounting for the regional context effect, our analysis confirmed regional mortality variability in mortality among older patients with septic shock. Mortality was influenced by whether ICU physicians are board-certified in intensive care medicine. These findings suggest that sufficient commitment in terms of time, intensity, and knowledge is crucial to reducing mortality in older patients with septic shock.</p>","PeriodicalId":73550,"journal":{"name":"JMA journal","volume":"8 3","pages":"708-717"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12329006/pdf/","citationCount":"0","resultStr":"{\"title\":\"Regional Differences and Mortality-associated Risk Factors among Older Patients with Septic Shock: Administrative Data Analysis with Multilevel Logistic Regression Modelling.\",\"authors\":\"Shinichiro Yoshida, Akira Babazono, Ning Liu, Reiko Yamao, Reiko Ishihara\",\"doi\":\"10.31662/jmaj.2024-0331\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Variations in intensive care unit (ICU) policies and physician characteristics influence mortality, potentially leading to regional differences in mortality rates. Previous studies have not specifically focused on septic shock or older patients and have lacked consideration of the context effect. We hypothesized that regional variability in mortality exists among older patients with septic shock and investigated factors associated with mortality.</p><p><strong>Methods: </strong>Administrative medical claims data were analyzed. Participants were enrolled from April 2015 to March 2020 in Fukuoka Prefecture, Japan. ICU physicians were classified based on board certification in intensive care medicine as either \\\"intensivists\\\" or \\\"ICU-dedicated physicians\\\". The primary outcome was 28-day mortality after ICU admission. Data from all ICUs in Fukuoka Prefecture and 9 secondary medical areas were analyzed. We calculated and compared the 28-day mortality rates across regions. Multilevel logistic regression analyses were conducted to adjust for the context effect.</p><p><strong>Results: </strong>Among the 1,238 participants, mortality across regions ranged from 18.3% to 41.4%. Based on multilevel logistic analyses, age, sex, postsurgical admission, and the number of ICU beds per intensivist were significantly associated with mortality. The adjusted odds ratio from the multilevel analysis for having no intensivists versus having ≥1 intensivist per 4 ICU beds was 1.99 (95% confidence interval 1.15-3.44, p = 0.01).</p><p><strong>Conclusions: </strong>After accounting for the regional context effect, our analysis confirmed regional mortality variability in mortality among older patients with septic shock. Mortality was influenced by whether ICU physicians are board-certified in intensive care medicine. These findings suggest that sufficient commitment in terms of time, intensity, and knowledge is crucial to reducing mortality in older patients with septic shock.</p>\",\"PeriodicalId\":73550,\"journal\":{\"name\":\"JMA journal\",\"volume\":\"8 3\",\"pages\":\"708-717\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12329006/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMA journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31662/jmaj.2024-0331\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMA journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31662/jmaj.2024-0331","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Regional Differences and Mortality-associated Risk Factors among Older Patients with Septic Shock: Administrative Data Analysis with Multilevel Logistic Regression Modelling.
Introduction: Variations in intensive care unit (ICU) policies and physician characteristics influence mortality, potentially leading to regional differences in mortality rates. Previous studies have not specifically focused on septic shock or older patients and have lacked consideration of the context effect. We hypothesized that regional variability in mortality exists among older patients with septic shock and investigated factors associated with mortality.
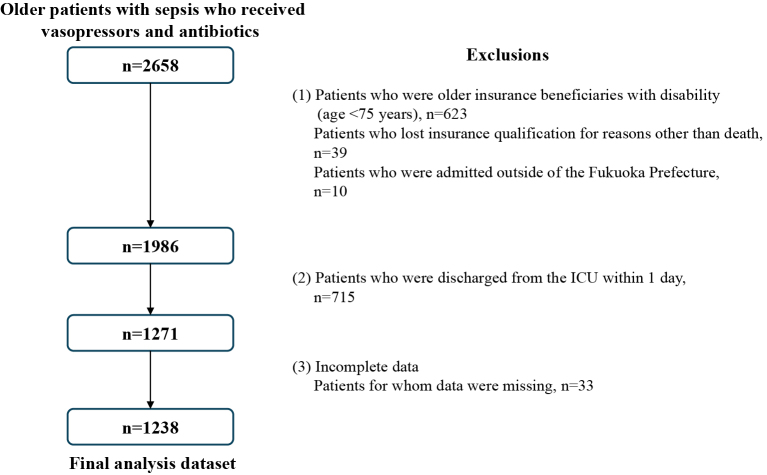
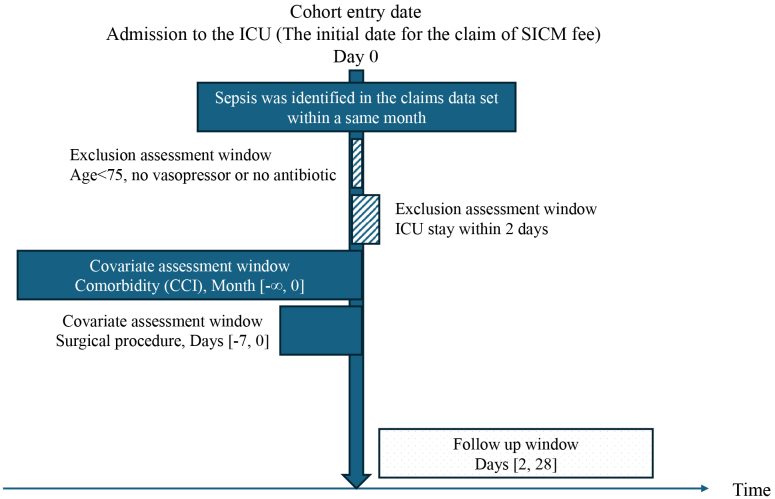
Methods: Administrative medical claims data were analyzed. Participants were enrolled from April 2015 to March 2020 in Fukuoka Prefecture, Japan. ICU physicians were classified based on board certification in intensive care medicine as either "intensivists" or "ICU-dedicated physicians". The primary outcome was 28-day mortality after ICU admission. Data from all ICUs in Fukuoka Prefecture and 9 secondary medical areas were analyzed. We calculated and compared the 28-day mortality rates across regions. Multilevel logistic regression analyses were conducted to adjust for the context effect.
Results: Among the 1,238 participants, mortality across regions ranged from 18.3% to 41.4%. Based on multilevel logistic analyses, age, sex, postsurgical admission, and the number of ICU beds per intensivist were significantly associated with mortality. The adjusted odds ratio from the multilevel analysis for having no intensivists versus having ≥1 intensivist per 4 ICU beds was 1.99 (95% confidence interval 1.15-3.44, p = 0.01).
Conclusions: After accounting for the regional context effect, our analysis confirmed regional mortality variability in mortality among older patients with septic shock. Mortality was influenced by whether ICU physicians are board-certified in intensive care medicine. These findings suggest that sufficient commitment in terms of time, intensity, and knowledge is crucial to reducing mortality in older patients with septic shock.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


