Jiali Ma, Changhao Cao, Chenqin Que, Jiayi Wan, Linkun Hu, Jie Li, Yixing Yu, Peng Wu, Chunhong Hu, Lingjie Wang, Mo Zhu
{"title":"动脉自旋标记和弥散张量成像-磁共振成像在无创评估同种异体肾移植功能障碍中的前瞻性评价。","authors":"Jiali Ma, Changhao Cao, Chenqin Que, Jiayi Wan, Linkun Hu, Jie Li, Yixing Yu, Peng Wu, Chunhong Hu, Lingjie Wang, Mo Zhu","doi":"10.21037/qims-2025-604","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal management strategy for end-stage renal disease is renal transplantation, graft function must be monitored regularly postoperatively. This cross-sectional study aimed to explore the value of combining functional magnetic resonance imaging (MRI) parameters with laboratory parameters in assessing chronic allograft dysfunction (CAD), and to compare whether a combined approach was superior to single-parameter indicators.</p><p><strong>Methods: </strong>A total of 86 subjects were enrolled in the study, of whom, 20 had stable renal function, and 66 had biopsy-confirmed CAD. Imaging was performed on a 1.5-T MRI system using T2-weighted imaging, arterial spin labeling (ASL), and diffusion tensor imaging (DTI). The serum creatinine, estimated glomerular filtration rate (eGFR), 24-hour urinary protein (24hUP), renal blood flow (RBF), and fractional anisotropy (FA) values of the subjects were measured. Correlation analysis was applied to assess MRI parameters' association with eGFR, while receiver operating characteristic (ROC) curves were used to evaluate the diagnostic efficacy of fMRI parameters and clinical parameters for CAD.</p><p><strong>Results: </strong>The subjects were categorized into CAD groups based on their eGFR levels. The control group had higher renal RBF [277.69±67.17 <i>vs.</i> 138.60 (99.54-193.51)] and FA values [cortex: 0.16 (0.14-0.16) <i>vs</i>. 0.13 (0.11-0.16); medulla: 0.32±0.06 <i>vs.</i> 0.24 (0.20-0.29)] than the CAD group (P<0.01). Cortical RBF decreased progressively across the CAD subgroups [group 1 (mild: 213.33±67.07) > group 2 (moderate: 151.14±53.21) > group 3 (severe: 92.89±35.62); all P<0.05]. Similarly, there was a gradual decrease in medullary FA across the CAD subgroups [group 1: 0.29±0.04; group 2: 0.24 (0.19-0.29); group 3: 0.20±0.06]. However, no statistically significant difference was found in medullary FA between groups 2 and 3 (P=0.102). The correlation analysis showed that cortical RBF and medullary FA were positively correlated with the eGFR in the CAD group (r=0.604, P<0.001; r=0.574, P<0.001). The combined RBF, medullary FA, 24hUP, and eGFR model (RBF-FA-24hUP-eGFR) had an area under the curve (AUC) of 0.95 [95% confidence interval (CI): 0.91-1.00], which was significantly better than the AUCs of the single indicators of 24hUP and medullary FA (AUC =0.78, 95% CI: 0.68-0.88; AUC =0.79, 95% CI: 0.69-0.89, P<0.05). Further, the combined RBF, medullary FA, and, 24hUP model (RBF-FA-24hUP) was significantly superior to single 24hUP in differentiating among the subgroups (all P<0.05). In the CAD subgroups, while the performance of RBF on its own was close to that of the RBF-FA-24hUP model, the AUC of the combined model showed an increasing trend compared with RBF. Notably, the RBF-FA-24hUP model (AUC =0.86, 95% CI: 0.76-0.97; P<0.001) also surpassed medullary FA alone (AUC =0.69, 95% CI: 0.54-0.85; P=0.023) in distinguishing between the subjects in group 2 and group 3 (P<0.05).</p><p><strong>Conclusions: </strong>In this study, two multiparametric MRI models (RBF-FA-24hUP-eGFR and RBF-FA-24hUP) were developed and shown to be superior to non-invasive CAD assessment tools. These models outperformed conventional single-parameter methods in diagnosis and moderate-to-severe subgroup stratification. To a certain extent, these models could prevent unnecessary puncture biopsies, and reduce the occurrence of complications such as bleeding and infection. RBF in particular and FA showed utility as non-invasive biomarkers for CAD and risk stratification.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 8","pages":"6882-6896"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12332621/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prospective evaluation of arterial spin labeling and diffusion tensor imaging-magnetic resonance imaging for the non-invasive assessment of renal allograft dysfunction.\",\"authors\":\"Jiali Ma, Changhao Cao, Chenqin Que, Jiayi Wan, Linkun Hu, Jie Li, Yixing Yu, Peng Wu, Chunhong Hu, Lingjie Wang, Mo Zhu\",\"doi\":\"10.21037/qims-2025-604\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The optimal management strategy for end-stage renal disease is renal transplantation, graft function must be monitored regularly postoperatively. This cross-sectional study aimed to explore the value of combining functional magnetic resonance imaging (MRI) parameters with laboratory parameters in assessing chronic allograft dysfunction (CAD), and to compare whether a combined approach was superior to single-parameter indicators.</p><p><strong>Methods: </strong>A total of 86 subjects were enrolled in the study, of whom, 20 had stable renal function, and 66 had biopsy-confirmed CAD. Imaging was performed on a 1.5-T MRI system using T2-weighted imaging, arterial spin labeling (ASL), and diffusion tensor imaging (DTI). The serum creatinine, estimated glomerular filtration rate (eGFR), 24-hour urinary protein (24hUP), renal blood flow (RBF), and fractional anisotropy (FA) values of the subjects were measured. Correlation analysis was applied to assess MRI parameters' association with eGFR, while receiver operating characteristic (ROC) curves were used to evaluate the diagnostic efficacy of fMRI parameters and clinical parameters for CAD.</p><p><strong>Results: </strong>The subjects were categorized into CAD groups based on their eGFR levels. The control group had higher renal RBF [277.69±67.17 <i>vs.</i> 138.60 (99.54-193.51)] and FA values [cortex: 0.16 (0.14-0.16) <i>vs</i>. 0.13 (0.11-0.16); medulla: 0.32±0.06 <i>vs.</i> 0.24 (0.20-0.29)] than the CAD group (P<0.01). Cortical RBF decreased progressively across the CAD subgroups [group 1 (mild: 213.33±67.07) > group 2 (moderate: 151.14±53.21) > group 3 (severe: 92.89±35.62); all P<0.05]. Similarly, there was a gradual decrease in medullary FA across the CAD subgroups [group 1: 0.29±0.04; group 2: 0.24 (0.19-0.29); group 3: 0.20±0.06]. However, no statistically significant difference was found in medullary FA between groups 2 and 3 (P=0.102). The correlation analysis showed that cortical RBF and medullary FA were positively correlated with the eGFR in the CAD group (r=0.604, P<0.001; r=0.574, P<0.001). The combined RBF, medullary FA, 24hUP, and eGFR model (RBF-FA-24hUP-eGFR) had an area under the curve (AUC) of 0.95 [95% confidence interval (CI): 0.91-1.00], which was significantly better than the AUCs of the single indicators of 24hUP and medullary FA (AUC =0.78, 95% CI: 0.68-0.88; AUC =0.79, 95% CI: 0.69-0.89, P<0.05). Further, the combined RBF, medullary FA, and, 24hUP model (RBF-FA-24hUP) was significantly superior to single 24hUP in differentiating among the subgroups (all P<0.05). In the CAD subgroups, while the performance of RBF on its own was close to that of the RBF-FA-24hUP model, the AUC of the combined model showed an increasing trend compared with RBF. Notably, the RBF-FA-24hUP model (AUC =0.86, 95% CI: 0.76-0.97; P<0.001) also surpassed medullary FA alone (AUC =0.69, 95% CI: 0.54-0.85; P=0.023) in distinguishing between the subjects in group 2 and group 3 (P<0.05).</p><p><strong>Conclusions: </strong>In this study, two multiparametric MRI models (RBF-FA-24hUP-eGFR and RBF-FA-24hUP) were developed and shown to be superior to non-invasive CAD assessment tools. These models outperformed conventional single-parameter methods in diagnosis and moderate-to-severe subgroup stratification. To a certain extent, these models could prevent unnecessary puncture biopsies, and reduce the occurrence of complications such as bleeding and infection. RBF in particular and FA showed utility as non-invasive biomarkers for CAD and risk stratification.</p>\",\"PeriodicalId\":54267,\"journal\":{\"name\":\"Quantitative Imaging in Medicine and Surgery\",\"volume\":\"15 8\",\"pages\":\"6882-6896\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12332621/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quantitative Imaging in Medicine and Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/qims-2025-604\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-604","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:终末期肾病的最佳治疗策略是肾移植,术后必须定期监测移植物功能。本横断面研究旨在探讨功能磁共振成像(MRI)参数与实验室参数联合评估慢性同种异体移植物功能障碍(CAD)的价值,并比较联合方法是否优于单一参数指标。方法:共纳入86例受试者,其中肾功能稳定者20例,活检证实冠心病者66例。在1.5 t MRI系统上使用t2加权成像、动脉自旋标记(ASL)和弥散张量成像(DTI)进行成像。测定受试者血清肌酐、估计肾小球滤过率(eGFR)、24小时尿蛋白(24hUP)、肾血流量(RBF)和分数各向异性(FA)值。采用相关性分析评价MRI参数与eGFR的相关性,采用受试者工作特征(ROC)曲线评价fMRI参数与临床参数对CAD的诊断效果。结果:根据受试者的eGFR水平将受试者分为CAD组。对照组肾RBF[277.69±67.17比138.60(99.54-193.51)]和FA值[皮质:0.16(0.14-0.16)比0.13(0.11-0.16)]较高;髓质:0.32±0.06 vs. 0.24(0.20-0.29)]比CAD组(P组2(中度:151.14±53.21)>组3(重度:92.89±35.62);结论:在本研究中,开发了两种多参数MRI模型(RBF-FA-24hUP- egfr和RBF-FA-24hUP),并证明其优于无创CAD评估工具。这些模型在诊断和中重度亚组分层方面优于传统的单参数方法。这些模型在一定程度上可以避免不必要的穿刺活检,减少出血、感染等并发症的发生。特别是RBF和FA显示了作为CAD和风险分层的非侵入性生物标志物的效用。
Prospective evaluation of arterial spin labeling and diffusion tensor imaging-magnetic resonance imaging for the non-invasive assessment of renal allograft dysfunction.
Background: The optimal management strategy for end-stage renal disease is renal transplantation, graft function must be monitored regularly postoperatively. This cross-sectional study aimed to explore the value of combining functional magnetic resonance imaging (MRI) parameters with laboratory parameters in assessing chronic allograft dysfunction (CAD), and to compare whether a combined approach was superior to single-parameter indicators.
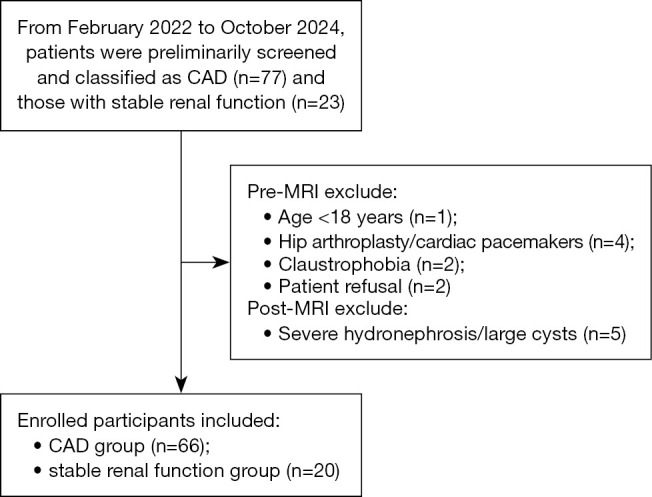
Methods: A total of 86 subjects were enrolled in the study, of whom, 20 had stable renal function, and 66 had biopsy-confirmed CAD. Imaging was performed on a 1.5-T MRI system using T2-weighted imaging, arterial spin labeling (ASL), and diffusion tensor imaging (DTI). The serum creatinine, estimated glomerular filtration rate (eGFR), 24-hour urinary protein (24hUP), renal blood flow (RBF), and fractional anisotropy (FA) values of the subjects were measured. Correlation analysis was applied to assess MRI parameters' association with eGFR, while receiver operating characteristic (ROC) curves were used to evaluate the diagnostic efficacy of fMRI parameters and clinical parameters for CAD.
Results: The subjects were categorized into CAD groups based on their eGFR levels. The control group had higher renal RBF [277.69±67.17 vs. 138.60 (99.54-193.51)] and FA values [cortex: 0.16 (0.14-0.16) vs. 0.13 (0.11-0.16); medulla: 0.32±0.06 vs. 0.24 (0.20-0.29)] than the CAD group (P<0.01). Cortical RBF decreased progressively across the CAD subgroups [group 1 (mild: 213.33±67.07) > group 2 (moderate: 151.14±53.21) > group 3 (severe: 92.89±35.62); all P<0.05]. Similarly, there was a gradual decrease in medullary FA across the CAD subgroups [group 1: 0.29±0.04; group 2: 0.24 (0.19-0.29); group 3: 0.20±0.06]. However, no statistically significant difference was found in medullary FA between groups 2 and 3 (P=0.102). The correlation analysis showed that cortical RBF and medullary FA were positively correlated with the eGFR in the CAD group (r=0.604, P<0.001; r=0.574, P<0.001). The combined RBF, medullary FA, 24hUP, and eGFR model (RBF-FA-24hUP-eGFR) had an area under the curve (AUC) of 0.95 [95% confidence interval (CI): 0.91-1.00], which was significantly better than the AUCs of the single indicators of 24hUP and medullary FA (AUC =0.78, 95% CI: 0.68-0.88; AUC =0.79, 95% CI: 0.69-0.89, P<0.05). Further, the combined RBF, medullary FA, and, 24hUP model (RBF-FA-24hUP) was significantly superior to single 24hUP in differentiating among the subgroups (all P<0.05). In the CAD subgroups, while the performance of RBF on its own was close to that of the RBF-FA-24hUP model, the AUC of the combined model showed an increasing trend compared with RBF. Notably, the RBF-FA-24hUP model (AUC =0.86, 95% CI: 0.76-0.97; P<0.001) also surpassed medullary FA alone (AUC =0.69, 95% CI: 0.54-0.85; P=0.023) in distinguishing between the subjects in group 2 and group 3 (P<0.05).
Conclusions: In this study, two multiparametric MRI models (RBF-FA-24hUP-eGFR and RBF-FA-24hUP) were developed and shown to be superior to non-invasive CAD assessment tools. These models outperformed conventional single-parameter methods in diagnosis and moderate-to-severe subgroup stratification. To a certain extent, these models could prevent unnecessary puncture biopsies, and reduce the occurrence of complications such as bleeding and infection. RBF in particular and FA showed utility as non-invasive biomarkers for CAD and risk stratification.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


