Bernadett Farkas, Peter Bacsur, Anita Bálint, Emese Ivány, Mariann Rutka, Anna Fábián, Zsófia Bősze, Renáta Bor, Zoltán Szepes, Klaudia Farkas, Tamás Molnár
{"title":"静脉皮质类固醇治疗难治性严重溃疡性结肠炎患者环孢素抢救治疗的短期和长期疗效。","authors":"Bernadett Farkas, Peter Bacsur, Anita Bálint, Emese Ivány, Mariann Rutka, Anna Fábián, Zsófia Bősze, Renáta Bor, Zoltán Szepes, Klaudia Farkas, Tamás Molnár","doi":"10.1177/17562848251361054","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Many patients with severe ulcerative colitis (UC) fail to respond to first-line corticosteroids and require second-line rescue therapy with cyclosporin (CsA) to avoid colectomy.</p><p><strong>Objectives: </strong>To assess the short- and long-term effectiveness and safety of CsA therapy.</p><p><strong>Design: </strong>A single-center, retrospective study was conducted, including patients who received IV CsA therapy for severe, steroid-refractory UC.</p><p><strong>Methods: </strong>Data on therapeutic response and adverse events (AEs) were reported. The Kaplan-Meier method was used to estimate colectomy-free survival rates. The incidence of inflammatory bowel disease flare-ups and the use of advanced therapies after CsA discontinuation were also assessed. Regression analyses were performed to identify predictors for therapeutic response, colectomy, and AEs with CsA.</p><p><strong>Results: </strong>A total of 92 UC patients (54.4% male, mean age: 40.0 ± 14.0 years) were included with the median follow-up time of 14 years (IQR: 7-18). Clinical response was achieved in 88.0%, and clinical remission was observed in 23.9% of patients after the median 6-day (IQR: 7-5) IV phase. A total of 40.7% of responders experienced clinical remission, whereas 13.6% had endoscopic remission at the time of CsA withdrawal (median after 5 months of therapy). Patients receiving concomitant immunomodulators were more likely to achieve clinical remission with CsA (<i>p</i> = 0.002; OR: 6.4). After CsA discontinuation, 23.5% of patients relapsed within 6 months, while 59.3% of patients were started on biologics. The probability of colectomy-free survival was 74.7%, 62.6%, 57.1%, and 45.6% at 1, 3, 5, and 14 years after CsA initiation. AEs were reported in 53.3% of patients, mainly hyperlipidaemia, hypertension, and infections. Hypoalbuminaemia (<35 g/L) at treatment initiation increased the risk of AEs (<i>p</i> = 0.03; OR: 0.4), whereas the occurrence of AEs was not associated with concomitant immunomodulator use (<i>p</i> = 0.9).</p><p><strong>Conclusion: </strong>CsA may be a potent therapeutic option to induce remission in steroid-refractory, severely active UC, and its effectiveness may be enhanced by the concomitant use of immunomodulators, without compromising safety.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251361054"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12334824/pdf/","citationCount":"0","resultStr":"{\"title\":\"Short- and longevity outcome of cyclosporin rescue therapy in severe ulcerative colitis refractory to intravenous corticosteroid treatment.\",\"authors\":\"Bernadett Farkas, Peter Bacsur, Anita Bálint, Emese Ivány, Mariann Rutka, Anna Fábián, Zsófia Bősze, Renáta Bor, Zoltán Szepes, Klaudia Farkas, Tamás Molnár\",\"doi\":\"10.1177/17562848251361054\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Many patients with severe ulcerative colitis (UC) fail to respond to first-line corticosteroids and require second-line rescue therapy with cyclosporin (CsA) to avoid colectomy.</p><p><strong>Objectives: </strong>To assess the short- and long-term effectiveness and safety of CsA therapy.</p><p><strong>Design: </strong>A single-center, retrospective study was conducted, including patients who received IV CsA therapy for severe, steroid-refractory UC.</p><p><strong>Methods: </strong>Data on therapeutic response and adverse events (AEs) were reported. The Kaplan-Meier method was used to estimate colectomy-free survival rates. The incidence of inflammatory bowel disease flare-ups and the use of advanced therapies after CsA discontinuation were also assessed. Regression analyses were performed to identify predictors for therapeutic response, colectomy, and AEs with CsA.</p><p><strong>Results: </strong>A total of 92 UC patients (54.4% male, mean age: 40.0 ± 14.0 years) were included with the median follow-up time of 14 years (IQR: 7-18). Clinical response was achieved in 88.0%, and clinical remission was observed in 23.9% of patients after the median 6-day (IQR: 7-5) IV phase. A total of 40.7% of responders experienced clinical remission, whereas 13.6% had endoscopic remission at the time of CsA withdrawal (median after 5 months of therapy). Patients receiving concomitant immunomodulators were more likely to achieve clinical remission with CsA (<i>p</i> = 0.002; OR: 6.4). After CsA discontinuation, 23.5% of patients relapsed within 6 months, while 59.3% of patients were started on biologics. The probability of colectomy-free survival was 74.7%, 62.6%, 57.1%, and 45.6% at 1, 3, 5, and 14 years after CsA initiation. AEs were reported in 53.3% of patients, mainly hyperlipidaemia, hypertension, and infections. Hypoalbuminaemia (<35 g/L) at treatment initiation increased the risk of AEs (<i>p</i> = 0.03; OR: 0.4), whereas the occurrence of AEs was not associated with concomitant immunomodulator use (<i>p</i> = 0.9).</p><p><strong>Conclusion: </strong>CsA may be a potent therapeutic option to induce remission in steroid-refractory, severely active UC, and its effectiveness may be enhanced by the concomitant use of immunomodulators, without compromising safety.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"18 \",\"pages\":\"17562848251361054\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12334824/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848251361054\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251361054","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Short- and longevity outcome of cyclosporin rescue therapy in severe ulcerative colitis refractory to intravenous corticosteroid treatment.
Background: Many patients with severe ulcerative colitis (UC) fail to respond to first-line corticosteroids and require second-line rescue therapy with cyclosporin (CsA) to avoid colectomy.
Objectives: To assess the short- and long-term effectiveness and safety of CsA therapy.
Design: A single-center, retrospective study was conducted, including patients who received IV CsA therapy for severe, steroid-refractory UC.
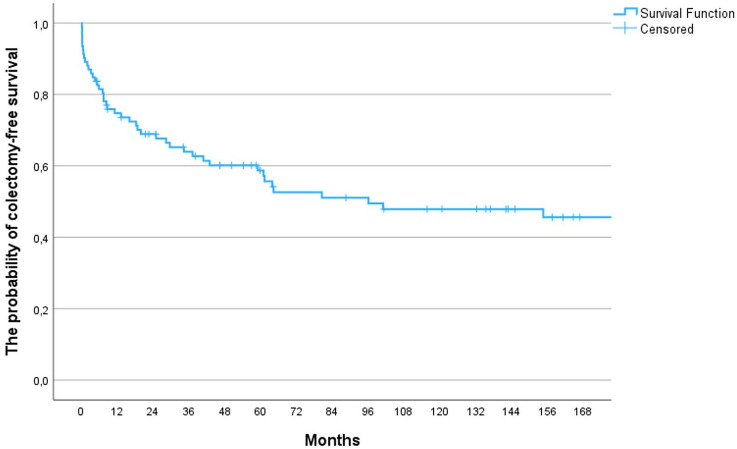
Methods: Data on therapeutic response and adverse events (AEs) were reported. The Kaplan-Meier method was used to estimate colectomy-free survival rates. The incidence of inflammatory bowel disease flare-ups and the use of advanced therapies after CsA discontinuation were also assessed. Regression analyses were performed to identify predictors for therapeutic response, colectomy, and AEs with CsA.
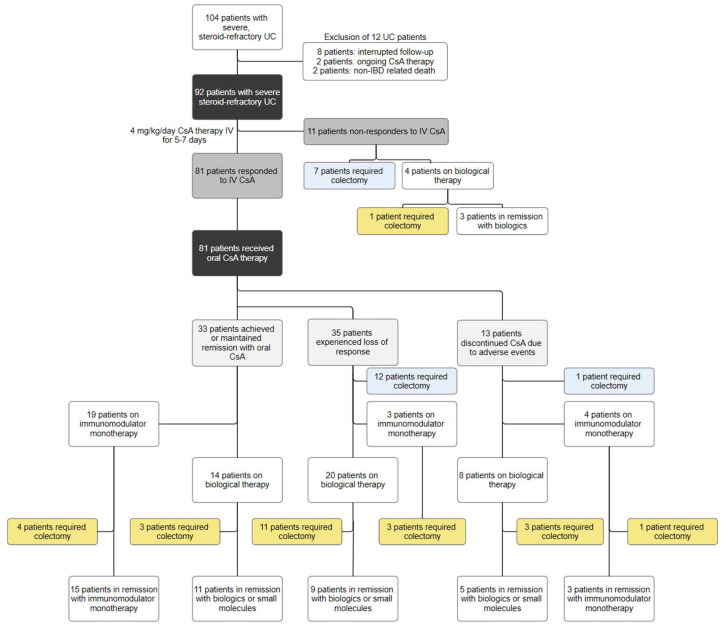
Results: A total of 92 UC patients (54.4% male, mean age: 40.0 ± 14.0 years) were included with the median follow-up time of 14 years (IQR: 7-18). Clinical response was achieved in 88.0%, and clinical remission was observed in 23.9% of patients after the median 6-day (IQR: 7-5) IV phase. A total of 40.7% of responders experienced clinical remission, whereas 13.6% had endoscopic remission at the time of CsA withdrawal (median after 5 months of therapy). Patients receiving concomitant immunomodulators were more likely to achieve clinical remission with CsA (p = 0.002; OR: 6.4). After CsA discontinuation, 23.5% of patients relapsed within 6 months, while 59.3% of patients were started on biologics. The probability of colectomy-free survival was 74.7%, 62.6%, 57.1%, and 45.6% at 1, 3, 5, and 14 years after CsA initiation. AEs were reported in 53.3% of patients, mainly hyperlipidaemia, hypertension, and infections. Hypoalbuminaemia (<35 g/L) at treatment initiation increased the risk of AEs (p = 0.03; OR: 0.4), whereas the occurrence of AEs was not associated with concomitant immunomodulator use (p = 0.9).
Conclusion: CsA may be a potent therapeutic option to induce remission in steroid-refractory, severely active UC, and its effectiveness may be enhanced by the concomitant use of immunomodulators, without compromising safety.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


