Maria Teresa Izquierdo de Francisco, Josep Navarro-Manchon, Oscar Cano Perez, Javier Navarrete Navarro, Carmen Arveras Martinez, Fransciso Javier Chorro Gasco, Luis Martinez-Dolz, Joaquin Osca Asensi
{"title":"使用farappulse系统隔离肺静脉时累及后壁。","authors":"Maria Teresa Izquierdo de Francisco, Josep Navarro-Manchon, Oscar Cano Perez, Javier Navarrete Navarro, Carmen Arveras Martinez, Fransciso Javier Chorro Gasco, Luis Martinez-Dolz, Joaquin Osca Asensi","doi":"10.1002/joa3.70171","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>First approved PFA (Pulsed-Field-Ablation) system for pulmonary vein isolation (PVI) has been Farapulse PFA system. The aim was to assess the characteristics of the lesion made by the Farapulse system and its influence on the clinical results.</p><p><strong>Methods: </strong>First 76 consecutive patients referred for PVI and treated with the Farapulse PFA system were included. A voltage and an activation map were performed before and after PVI. An imaginary middle line was measured between the two carinas. Fusion on the posterior wall was defined when the contralateral ablation areas were connected. We arbitrarily defined a narrow corridor as one that measured < 20 mm of healthy tissue (voltage > 0.5 mV).</p><p><strong>Results: </strong>Post-PVI mapping revealed an unexpected narrow corridor in the posterior wall in 12 (15%) and fusion in 18 (23%) patients. The multivariate analysis revealed that the only independent predictor was the length of the middle inter-carinas line. The length of the middle posterior line was significantly shorter in patients with affectation of the posterior wall (62 ± 2 vs. 71 ± 3 mm, <i>p</i> = 0.0001). ROC curve showed that a middle line cutoff value of 65 mm offered a sensitivity and specificity of 80% and 70% (AUC: 0.82; 95% CI: 0.59-0.84). A corridor < 10 mm is associated with slow conduction velocity below 0.7 m/s, but narrow corridor or fusion were not associated with atrial fibrillation recurrences.</p><p><strong>Conclusions: </strong>30 (40%) patients showed narrow corridor or fusion on the posterior wall. The only independent predictor was the length of the middle inter-carina line.</p>","PeriodicalId":15174,"journal":{"name":"Journal of Arrhythmia","volume":"41 4","pages":"e70171"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331866/pdf/","citationCount":"0","resultStr":"{\"title\":\"Posterior Wall Involvement During Pulmonary Vein Isolation Using the Farapulse System.\",\"authors\":\"Maria Teresa Izquierdo de Francisco, Josep Navarro-Manchon, Oscar Cano Perez, Javier Navarrete Navarro, Carmen Arveras Martinez, Fransciso Javier Chorro Gasco, Luis Martinez-Dolz, Joaquin Osca Asensi\",\"doi\":\"10.1002/joa3.70171\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>First approved PFA (Pulsed-Field-Ablation) system for pulmonary vein isolation (PVI) has been Farapulse PFA system. The aim was to assess the characteristics of the lesion made by the Farapulse system and its influence on the clinical results.</p><p><strong>Methods: </strong>First 76 consecutive patients referred for PVI and treated with the Farapulse PFA system were included. A voltage and an activation map were performed before and after PVI. An imaginary middle line was measured between the two carinas. Fusion on the posterior wall was defined when the contralateral ablation areas were connected. We arbitrarily defined a narrow corridor as one that measured < 20 mm of healthy tissue (voltage > 0.5 mV).</p><p><strong>Results: </strong>Post-PVI mapping revealed an unexpected narrow corridor in the posterior wall in 12 (15%) and fusion in 18 (23%) patients. The multivariate analysis revealed that the only independent predictor was the length of the middle inter-carinas line. The length of the middle posterior line was significantly shorter in patients with affectation of the posterior wall (62 ± 2 vs. 71 ± 3 mm, <i>p</i> = 0.0001). ROC curve showed that a middle line cutoff value of 65 mm offered a sensitivity and specificity of 80% and 70% (AUC: 0.82; 95% CI: 0.59-0.84). A corridor < 10 mm is associated with slow conduction velocity below 0.7 m/s, but narrow corridor or fusion were not associated with atrial fibrillation recurrences.</p><p><strong>Conclusions: </strong>30 (40%) patients showed narrow corridor or fusion on the posterior wall. The only independent predictor was the length of the middle inter-carina line.</p>\",\"PeriodicalId\":15174,\"journal\":{\"name\":\"Journal of Arrhythmia\",\"volume\":\"41 4\",\"pages\":\"e70171\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331866/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Arrhythmia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/joa3.70171\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Arrhythmia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/joa3.70171","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:第一个批准用于肺静脉隔离(PVI)的PFA(脉冲场消融)系统是Farapulse PFA系统。目的是评估Farapulse系统病变的特征及其对临床结果的影响。方法:采用Farapulse PFA系统治疗PVI患者76例。PVI前后分别测量电压和激活图。在两个隆穴之间测量了一条假想的中线。当对侧消融区连接时,确定后壁融合。我们任意定义了一个狭窄的走廊,测量0.5毫伏)。结果:pvi后定位显示12例(15%)患者后壁出现意外狭窄通道,18例(23%)患者融合。多变量分析显示,唯一的独立预测因子是中间隆突线的长度。后壁畸形患者的后中线长度明显较短(62±2 vs 71±3 mm, p = 0.0001)。ROC曲线显示,65 mm的中线截断值的敏感性和特异性分别为80%和70% (AUC: 0.82;95% ci: 0.59-0.84)。结论:30例(40%)患者表现为后壁狭窄或融合。唯一的独立预测因子是中间隆突线的长度。
Posterior Wall Involvement During Pulmonary Vein Isolation Using the Farapulse System.
Background: First approved PFA (Pulsed-Field-Ablation) system for pulmonary vein isolation (PVI) has been Farapulse PFA system. The aim was to assess the characteristics of the lesion made by the Farapulse system and its influence on the clinical results.
Methods: First 76 consecutive patients referred for PVI and treated with the Farapulse PFA system were included. A voltage and an activation map were performed before and after PVI. An imaginary middle line was measured between the two carinas. Fusion on the posterior wall was defined when the contralateral ablation areas were connected. We arbitrarily defined a narrow corridor as one that measured < 20 mm of healthy tissue (voltage > 0.5 mV).
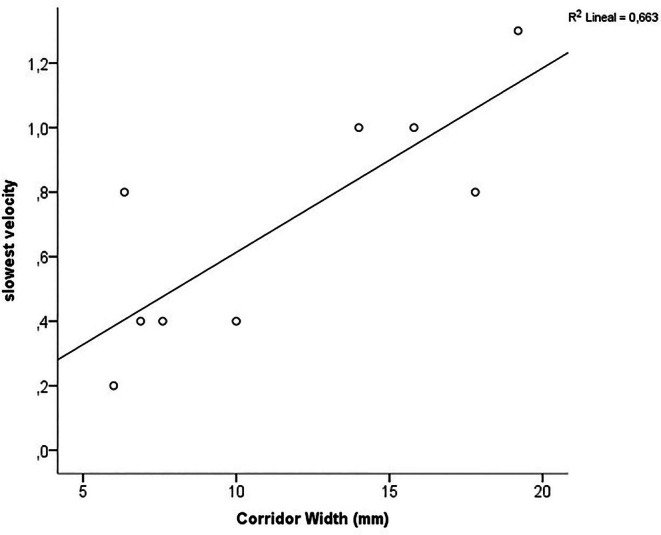
Results: Post-PVI mapping revealed an unexpected narrow corridor in the posterior wall in 12 (15%) and fusion in 18 (23%) patients. The multivariate analysis revealed that the only independent predictor was the length of the middle inter-carinas line. The length of the middle posterior line was significantly shorter in patients with affectation of the posterior wall (62 ± 2 vs. 71 ± 3 mm, p = 0.0001). ROC curve showed that a middle line cutoff value of 65 mm offered a sensitivity and specificity of 80% and 70% (AUC: 0.82; 95% CI: 0.59-0.84). A corridor < 10 mm is associated with slow conduction velocity below 0.7 m/s, but narrow corridor or fusion were not associated with atrial fibrillation recurrences.
Conclusions: 30 (40%) patients showed narrow corridor or fusion on the posterior wall. The only independent predictor was the length of the middle inter-carina line.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


