{"title":"继发于高胆红素血症的远端肾小管酸中毒。","authors":"Fawzi Srour, Aline Pourcelet, Ishak Beklevic, Guillaume Benoit, Serge Treille de Grandsaigne, Nathan Neveux","doi":"10.12890/2025_005661","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bile cast nephropathy (BCN) is a rare and often overlooked cause of acute kidney injury (AKI), usually seen in the context of severe hyperbilirubinemia. It results from the deposition of bile pigments and bile casts in renal tubules, specifically distal and collector tubules, leading to obstruction and direct tubular toxicity.</p><p><strong>Case description: </strong>We describe the case of 49-year-old male who presented with severe jaundice and oliguric AKI. With the gradual resolution of liver dysfunction, the patient's kidney function also improved. However, during the recovery phase, the patient developed persistent hypokalaemia and normal anion gap metabolic acidosis. Further work-up was consistent with distal renal tubular acidosis (dRTA).</p><p><strong>Discussion: </strong>While BCN is being increasingly recognized in patients with cholestatic liver diseases, complications arising during the recovery phase - particularly acid-base disturbances like dRTA - are rarely reported. In this case, the onset of dRTA during renal recovery may reflect delayed or selective tubular healing after bile-induced injury. This case highlights the importance of continued monitoring for renal tubular defects even after apparent improvement in glomerular function.</p><p><strong>Conclusion: </strong>This case emphasizes the need to consider dRTA as a potential complication in patients recovering from BCN. Close follow-up of electrolyte and acid-base parameters is advised during renal recovery, especially in the presence of persistent hypokalaemia.</p><p><strong>Learning points: </strong>Bile cast nephropathy (BCN) is an under-recognized cause of acute kidney injury (AKI) in patients with severe hyperbilirubinemia and should be considered in the differential diagnosis of AKI in jaundiced patients.Distal renal tubular acidosis (dRTA) can emerge during the recovery phase of BCN-related AKI, possibly due to tubular dysfunction from bile-induced injury, highlighting the need for close metabolic monitoring after renal recovery.The co-occurrence of BCN and dRTA emphasizes the importance of serial electrolyte assessments and acid-base evaluation in jaundiced patients with AKI, even after apparent improvement in renal function.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 8","pages":"005661"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331275/pdf/","citationCount":"0","resultStr":"{\"title\":\"Distal Renal Tubular Acidosis Secondary to Hyperbilirubinemia.\",\"authors\":\"Fawzi Srour, Aline Pourcelet, Ishak Beklevic, Guillaume Benoit, Serge Treille de Grandsaigne, Nathan Neveux\",\"doi\":\"10.12890/2025_005661\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Bile cast nephropathy (BCN) is a rare and often overlooked cause of acute kidney injury (AKI), usually seen in the context of severe hyperbilirubinemia. It results from the deposition of bile pigments and bile casts in renal tubules, specifically distal and collector tubules, leading to obstruction and direct tubular toxicity.</p><p><strong>Case description: </strong>We describe the case of 49-year-old male who presented with severe jaundice and oliguric AKI. With the gradual resolution of liver dysfunction, the patient's kidney function also improved. However, during the recovery phase, the patient developed persistent hypokalaemia and normal anion gap metabolic acidosis. Further work-up was consistent with distal renal tubular acidosis (dRTA).</p><p><strong>Discussion: </strong>While BCN is being increasingly recognized in patients with cholestatic liver diseases, complications arising during the recovery phase - particularly acid-base disturbances like dRTA - are rarely reported. In this case, the onset of dRTA during renal recovery may reflect delayed or selective tubular healing after bile-induced injury. This case highlights the importance of continued monitoring for renal tubular defects even after apparent improvement in glomerular function.</p><p><strong>Conclusion: </strong>This case emphasizes the need to consider dRTA as a potential complication in patients recovering from BCN. Close follow-up of electrolyte and acid-base parameters is advised during renal recovery, especially in the presence of persistent hypokalaemia.</p><p><strong>Learning points: </strong>Bile cast nephropathy (BCN) is an under-recognized cause of acute kidney injury (AKI) in patients with severe hyperbilirubinemia and should be considered in the differential diagnosis of AKI in jaundiced patients.Distal renal tubular acidosis (dRTA) can emerge during the recovery phase of BCN-related AKI, possibly due to tubular dysfunction from bile-induced injury, highlighting the need for close metabolic monitoring after renal recovery.The co-occurrence of BCN and dRTA emphasizes the importance of serial electrolyte assessments and acid-base evaluation in jaundiced patients with AKI, even after apparent improvement in renal function.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 8\",\"pages\":\"005661\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331275/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005661\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005661","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Distal Renal Tubular Acidosis Secondary to Hyperbilirubinemia.
Introduction: Bile cast nephropathy (BCN) is a rare and often overlooked cause of acute kidney injury (AKI), usually seen in the context of severe hyperbilirubinemia. It results from the deposition of bile pigments and bile casts in renal tubules, specifically distal and collector tubules, leading to obstruction and direct tubular toxicity.
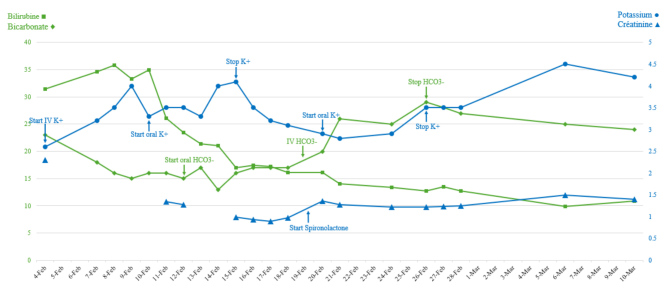
Case description: We describe the case of 49-year-old male who presented with severe jaundice and oliguric AKI. With the gradual resolution of liver dysfunction, the patient's kidney function also improved. However, during the recovery phase, the patient developed persistent hypokalaemia and normal anion gap metabolic acidosis. Further work-up was consistent with distal renal tubular acidosis (dRTA).
Discussion: While BCN is being increasingly recognized in patients with cholestatic liver diseases, complications arising during the recovery phase - particularly acid-base disturbances like dRTA - are rarely reported. In this case, the onset of dRTA during renal recovery may reflect delayed or selective tubular healing after bile-induced injury. This case highlights the importance of continued monitoring for renal tubular defects even after apparent improvement in glomerular function.
Conclusion: This case emphasizes the need to consider dRTA as a potential complication in patients recovering from BCN. Close follow-up of electrolyte and acid-base parameters is advised during renal recovery, especially in the presence of persistent hypokalaemia.
Learning points: Bile cast nephropathy (BCN) is an under-recognized cause of acute kidney injury (AKI) in patients with severe hyperbilirubinemia and should be considered in the differential diagnosis of AKI in jaundiced patients.Distal renal tubular acidosis (dRTA) can emerge during the recovery phase of BCN-related AKI, possibly due to tubular dysfunction from bile-induced injury, highlighting the need for close metabolic monitoring after renal recovery.The co-occurrence of BCN and dRTA emphasizes the importance of serial electrolyte assessments and acid-base evaluation in jaundiced patients with AKI, even after apparent improvement in renal function.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


