Simone Burgener-Enderli, Andreas Schmitt, Stefano Bassetti, Mark Kirsch
{"title":"模拟过敏性血管水肿的上腔静脉综合征:对纵隔b细胞淋巴瘤的过敏反应的诊断奥德赛。","authors":"Simone Burgener-Enderli, Andreas Schmitt, Stefano Bassetti, Mark Kirsch","doi":"10.12890/2025_005577","DOIUrl":null,"url":null,"abstract":"<p><p>An 18-year-old woman presented to her general practitioner with a history of non-itching facial swelling, erythematous skin rash and a slightly coarse voice for a few days. She denied dyspnoea, B-symptoms and pain. Physical examination revealed generalized facial and neck swelling not involving the tongue or the oral mucous membranes. There was no lymphadenopathy. These findings resulted in the diagnosis of allergic angioedema and in oral treatment with corticosteroids and antihistamines. The swelling responded partially but reoccurred with dose reduction of the corticosteroids. Outpatient referrals to a dermatologist, an endocrinologist and a rheumatologist resulted in confirmation of the diagnosis of allergic angioedema, suspected iatrogenic Cushing syndrome and possible connective tissue disease, respectively. Three months after the first outpatient presentation the patient was admitted to our hospital with severe fatigue and left-sided chest pain. The clinical examination showed the known facial and neck swelling- and a sinus tachycardia (120 bpm) without any fever. Furthermore, the neck swelling seemed to be slightly asymmetrical. This was accompanied by leucocytosis, elevated C-reactive protein, and lactate dehydrogenase. An electrocardiogram showed sinus tachycardia (120/min) with a S1Q3-type. An ultrasound of the neck showed thrombosis of the left jugular vein. Subsequent computed tomography scan of the chest revealed a large mediastinal mass causing acute superior vena cava syndrome. Mediastinal large B-cell lymphoma was confirmed by biopsy. The patient underwent six cycles of DA-R-EPOCH (rituximab, etoposide, prednisolone, vincristine, cyclophosphamide, doxorubicin). Treatment resulted in complete response.</p><p><strong>Learning points: </strong>Vena cava superior syndrome is caused in over 60% of the cases by malignancies (bronchogenic carcinoma, lymphoma, germ cell tumour).Facial swelling, plethora of the upper chest without itchiness and hoarseness are classical symptoms of thoracic central venous obstruction.At every patient visit open-minded clinical reasoning should be used to avoid anchoring bias.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 8","pages":"005577"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331284/pdf/","citationCount":"0","resultStr":"{\"title\":\"Superior Vena Cava Syndrome Mimicking an Allergic Angioedema: A Diagnostic Odyssey from Allergic Reaction to Mediastinal B-Cell Lymphoma.\",\"authors\":\"Simone Burgener-Enderli, Andreas Schmitt, Stefano Bassetti, Mark Kirsch\",\"doi\":\"10.12890/2025_005577\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>An 18-year-old woman presented to her general practitioner with a history of non-itching facial swelling, erythematous skin rash and a slightly coarse voice for a few days. She denied dyspnoea, B-symptoms and pain. Physical examination revealed generalized facial and neck swelling not involving the tongue or the oral mucous membranes. There was no lymphadenopathy. These findings resulted in the diagnosis of allergic angioedema and in oral treatment with corticosteroids and antihistamines. The swelling responded partially but reoccurred with dose reduction of the corticosteroids. Outpatient referrals to a dermatologist, an endocrinologist and a rheumatologist resulted in confirmation of the diagnosis of allergic angioedema, suspected iatrogenic Cushing syndrome and possible connective tissue disease, respectively. Three months after the first outpatient presentation the patient was admitted to our hospital with severe fatigue and left-sided chest pain. The clinical examination showed the known facial and neck swelling- and a sinus tachycardia (120 bpm) without any fever. Furthermore, the neck swelling seemed to be slightly asymmetrical. This was accompanied by leucocytosis, elevated C-reactive protein, and lactate dehydrogenase. An electrocardiogram showed sinus tachycardia (120/min) with a S1Q3-type. An ultrasound of the neck showed thrombosis of the left jugular vein. Subsequent computed tomography scan of the chest revealed a large mediastinal mass causing acute superior vena cava syndrome. Mediastinal large B-cell lymphoma was confirmed by biopsy. The patient underwent six cycles of DA-R-EPOCH (rituximab, etoposide, prednisolone, vincristine, cyclophosphamide, doxorubicin). Treatment resulted in complete response.</p><p><strong>Learning points: </strong>Vena cava superior syndrome is caused in over 60% of the cases by malignancies (bronchogenic carcinoma, lymphoma, germ cell tumour).Facial swelling, plethora of the upper chest without itchiness and hoarseness are classical symptoms of thoracic central venous obstruction.At every patient visit open-minded clinical reasoning should be used to avoid anchoring bias.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 8\",\"pages\":\"005577\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331284/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005577\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005577","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Superior Vena Cava Syndrome Mimicking an Allergic Angioedema: A Diagnostic Odyssey from Allergic Reaction to Mediastinal B-Cell Lymphoma.
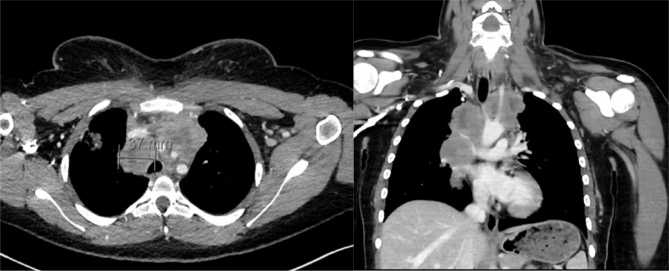
An 18-year-old woman presented to her general practitioner with a history of non-itching facial swelling, erythematous skin rash and a slightly coarse voice for a few days. She denied dyspnoea, B-symptoms and pain. Physical examination revealed generalized facial and neck swelling not involving the tongue or the oral mucous membranes. There was no lymphadenopathy. These findings resulted in the diagnosis of allergic angioedema and in oral treatment with corticosteroids and antihistamines. The swelling responded partially but reoccurred with dose reduction of the corticosteroids. Outpatient referrals to a dermatologist, an endocrinologist and a rheumatologist resulted in confirmation of the diagnosis of allergic angioedema, suspected iatrogenic Cushing syndrome and possible connective tissue disease, respectively. Three months after the first outpatient presentation the patient was admitted to our hospital with severe fatigue and left-sided chest pain. The clinical examination showed the known facial and neck swelling- and a sinus tachycardia (120 bpm) without any fever. Furthermore, the neck swelling seemed to be slightly asymmetrical. This was accompanied by leucocytosis, elevated C-reactive protein, and lactate dehydrogenase. An electrocardiogram showed sinus tachycardia (120/min) with a S1Q3-type. An ultrasound of the neck showed thrombosis of the left jugular vein. Subsequent computed tomography scan of the chest revealed a large mediastinal mass causing acute superior vena cava syndrome. Mediastinal large B-cell lymphoma was confirmed by biopsy. The patient underwent six cycles of DA-R-EPOCH (rituximab, etoposide, prednisolone, vincristine, cyclophosphamide, doxorubicin). Treatment resulted in complete response.
Learning points: Vena cava superior syndrome is caused in over 60% of the cases by malignancies (bronchogenic carcinoma, lymphoma, germ cell tumour).Facial swelling, plethora of the upper chest without itchiness and hoarseness are classical symptoms of thoracic central venous obstruction.At every patient visit open-minded clinical reasoning should be used to avoid anchoring bias.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


