Luke D Hunter, Simon Poerstamper, Philip G Herbst, Anton F Doubell, Colette Pienaar, Jantjie J Taljaard, Hans Prozesky, Jacques J Janson, Alfonso Jk Pecoraro
{"title":"巴尔通体心内膜炎:在非洲流行地区血培养阴性心内膜炎的复杂诊断。","authors":"Luke D Hunter, Simon Poerstamper, Philip G Herbst, Anton F Doubell, Colette Pienaar, Jantjie J Taljaard, Hans Prozesky, Jacques J Janson, Alfonso Jk Pecoraro","doi":"10.1136/openhrt-2025-003463","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong><i>Bartonella</i> species are an important emerging cause of blood culture-negative endocarditis (BCNE). The diagnosis requires serology by indirect immunofluorescence assay (IFA) and PCR testing on blood and/or tissue. Access to the guideline-referenced in-house IFA is limited in Africa and a commercially available IFA is used to identify patients with <i>Bartonella</i> spp. infection in our region. Prior study in South Africa has highlighted a high seroprevalence of <i>Bartonella</i> spp. in the general population. It is unclear how to incorporate these factors into the diagnostic thinking when interpreting a positive IFA result in a patient with BCNE. We explore these important knowledge gaps in a cohort of 31 patients with <i>Bartonella</i> endocarditis.</p><p><strong>Methods and results: </strong>Data from the Tygerberg Endocarditis Cohort Study were evaluated between October 2019 and May 2023. Continuous variables were reported as mean with SD if normally distributed, alternatively as median with IQR. Categorical variables were reported as counts and percentages. A Kaplan-Meier curve will be used to depict the mortality rate of operated versus unoperated patients. The mean age (±SD) was 38±9 years, 70.9% were male, 25.8% were either homeless or lived in informal housing, 70.9% were unemployed, 54.8% had an underlying alcohol-use disorder and 25.8% were HIV positive. Blood serology was positive (IgG titre ≥1:256) in 96.7% of patients with available sera. Valvular tissue was available for PCR testing in 18 cases. Of these, <i>Bartonella quintana</i> was identified in 16 cases and <i>Bartonella henselae</i> in one case. None of the cases with both serology and valve PCR data had negative serology. No cases of blood culture-positive endocarditis (BCPE) had a positive PCR for <i>Bartonella</i> spp. The most common isolated valve lesion on echocardiography was severe aortic regurgitation (43.3%). The 1-month and 6-month mortality in the operated cohort was 0% and 4.5%, respectively.</p><p><strong>Discussion: </strong><i>Bartonella quintana</i> is the most common cause of BCNE accounting for 49.2% of cases at our centre. None of the PCR-proven cases of <i>Bartonella</i> endocarditis had negative serology, which suggests that the test has a high negative predictive value. The current guideline diagnostic titre of ≥1:800 is assay dependent and is not generalisable to alternative, commercially available, assays. Crucially, none of the BCPE cases with available PCR on valve tissue had a positive PCR for <i>Bartonella</i> spp, suggesting a positive valve PCR is definitive evidence of true infection in an endemic region. The specific clinical, echocardiographic and mortality data were consistent with the reported literature and characterised a subacute, but ultimately destructive endocarditis with a high embolic risk and underscores the need for early surgical intervention.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12336616/pdf/","citationCount":"0","resultStr":"{\"title\":\"<i>Bartonella</i> endocarditis: a complex diagnosis of blood culture-negative endocarditis in an endemic region of Africa.\",\"authors\":\"Luke D Hunter, Simon Poerstamper, Philip G Herbst, Anton F Doubell, Colette Pienaar, Jantjie J Taljaard, Hans Prozesky, Jacques J Janson, Alfonso Jk Pecoraro\",\"doi\":\"10.1136/openhrt-2025-003463\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong><i>Bartonella</i> species are an important emerging cause of blood culture-negative endocarditis (BCNE). The diagnosis requires serology by indirect immunofluorescence assay (IFA) and PCR testing on blood and/or tissue. Access to the guideline-referenced in-house IFA is limited in Africa and a commercially available IFA is used to identify patients with <i>Bartonella</i> spp. infection in our region. Prior study in South Africa has highlighted a high seroprevalence of <i>Bartonella</i> spp. in the general population. It is unclear how to incorporate these factors into the diagnostic thinking when interpreting a positive IFA result in a patient with BCNE. We explore these important knowledge gaps in a cohort of 31 patients with <i>Bartonella</i> endocarditis.</p><p><strong>Methods and results: </strong>Data from the Tygerberg Endocarditis Cohort Study were evaluated between October 2019 and May 2023. Continuous variables were reported as mean with SD if normally distributed, alternatively as median with IQR. Categorical variables were reported as counts and percentages. A Kaplan-Meier curve will be used to depict the mortality rate of operated versus unoperated patients. The mean age (±SD) was 38±9 years, 70.9% were male, 25.8% were either homeless or lived in informal housing, 70.9% were unemployed, 54.8% had an underlying alcohol-use disorder and 25.8% were HIV positive. Blood serology was positive (IgG titre ≥1:256) in 96.7% of patients with available sera. Valvular tissue was available for PCR testing in 18 cases. Of these, <i>Bartonella quintana</i> was identified in 16 cases and <i>Bartonella henselae</i> in one case. None of the cases with both serology and valve PCR data had negative serology. No cases of blood culture-positive endocarditis (BCPE) had a positive PCR for <i>Bartonella</i> spp. The most common isolated valve lesion on echocardiography was severe aortic regurgitation (43.3%). The 1-month and 6-month mortality in the operated cohort was 0% and 4.5%, respectively.</p><p><strong>Discussion: </strong><i>Bartonella quintana</i> is the most common cause of BCNE accounting for 49.2% of cases at our centre. None of the PCR-proven cases of <i>Bartonella</i> endocarditis had negative serology, which suggests that the test has a high negative predictive value. The current guideline diagnostic titre of ≥1:800 is assay dependent and is not generalisable to alternative, commercially available, assays. Crucially, none of the BCPE cases with available PCR on valve tissue had a positive PCR for <i>Bartonella</i> spp, suggesting a positive valve PCR is definitive evidence of true infection in an endemic region. The specific clinical, echocardiographic and mortality data were consistent with the reported literature and characterised a subacute, but ultimately destructive endocarditis with a high embolic risk and underscores the need for early surgical intervention.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12336616/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2025-003463\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003463","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Bartonella endocarditis: a complex diagnosis of blood culture-negative endocarditis in an endemic region of Africa.
Introduction: Bartonella species are an important emerging cause of blood culture-negative endocarditis (BCNE). The diagnosis requires serology by indirect immunofluorescence assay (IFA) and PCR testing on blood and/or tissue. Access to the guideline-referenced in-house IFA is limited in Africa and a commercially available IFA is used to identify patients with Bartonella spp. infection in our region. Prior study in South Africa has highlighted a high seroprevalence of Bartonella spp. in the general population. It is unclear how to incorporate these factors into the diagnostic thinking when interpreting a positive IFA result in a patient with BCNE. We explore these important knowledge gaps in a cohort of 31 patients with Bartonella endocarditis.
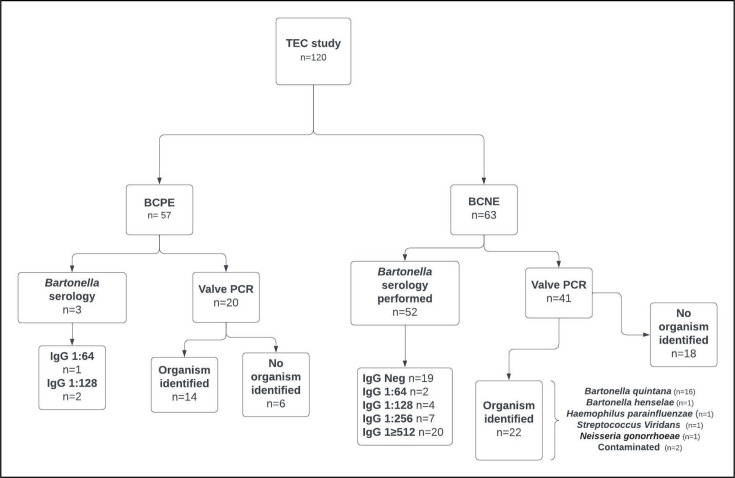
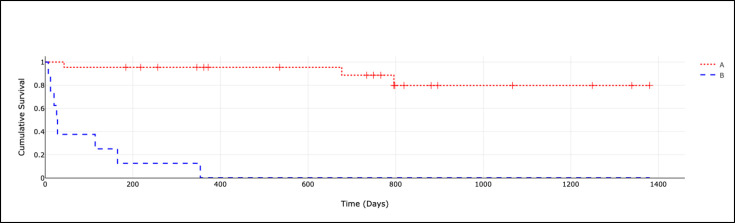
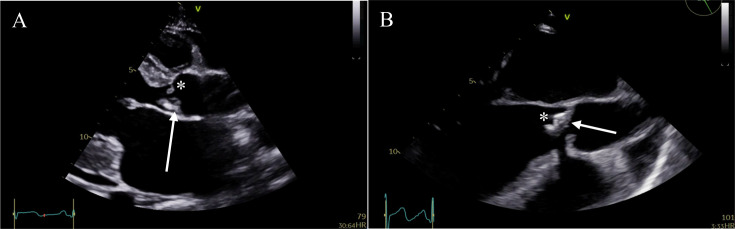
Methods and results: Data from the Tygerberg Endocarditis Cohort Study were evaluated between October 2019 and May 2023. Continuous variables were reported as mean with SD if normally distributed, alternatively as median with IQR. Categorical variables were reported as counts and percentages. A Kaplan-Meier curve will be used to depict the mortality rate of operated versus unoperated patients. The mean age (±SD) was 38±9 years, 70.9% were male, 25.8% were either homeless or lived in informal housing, 70.9% were unemployed, 54.8% had an underlying alcohol-use disorder and 25.8% were HIV positive. Blood serology was positive (IgG titre ≥1:256) in 96.7% of patients with available sera. Valvular tissue was available for PCR testing in 18 cases. Of these, Bartonella quintana was identified in 16 cases and Bartonella henselae in one case. None of the cases with both serology and valve PCR data had negative serology. No cases of blood culture-positive endocarditis (BCPE) had a positive PCR for Bartonella spp. The most common isolated valve lesion on echocardiography was severe aortic regurgitation (43.3%). The 1-month and 6-month mortality in the operated cohort was 0% and 4.5%, respectively.
Discussion: Bartonella quintana is the most common cause of BCNE accounting for 49.2% of cases at our centre. None of the PCR-proven cases of Bartonella endocarditis had negative serology, which suggests that the test has a high negative predictive value. The current guideline diagnostic titre of ≥1:800 is assay dependent and is not generalisable to alternative, commercially available, assays. Crucially, none of the BCPE cases with available PCR on valve tissue had a positive PCR for Bartonella spp, suggesting a positive valve PCR is definitive evidence of true infection in an endemic region. The specific clinical, echocardiographic and mortality data were consistent with the reported literature and characterised a subacute, but ultimately destructive endocarditis with a high embolic risk and underscores the need for early surgical intervention.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


