Yap-Hang Will Chan, Hoi-Ying Li, Hung-Fat Tse, Claire A Martin
{"title":"高频低潮气量通气提高心房颤动射频导管消融的长期成功:一项荟萃分析。","authors":"Yap-Hang Will Chan, Hoi-Ying Li, Hung-Fat Tse, Claire A Martin","doi":"10.1093/ehjopen/oeaf088","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>High-frequency low-tidal volume (HFLTV) ventilation may improve catheter stability and enhance procedural success in radiofrequency (RF) catheter ablation of atrial fibrillation (AF). Long-term findings remained unclear.</p><p><strong>Methods and results: </strong>We conducted a meta-analysis that included all studies that directly compared AF patients who underwent RF ablation under HFLTV compared with standard ventilation. Primary outcomes included acute first-pass pulmonary vein isolation (PVI) and long-term recurrence of AF/atrial arrhythmias after 12 months. Secondary outcomes included total procedure duration, ablation time, and RF time, with pooled standardized mean difference derived using the inverse variance method. Five cohort studies (publication period: 2019-2024) were identified and included in the meta-analysis (final sample: HFLTV <i>n</i> = 460 vs. standard ventilation <i>n</i> = 705). High-frequency low-tidal volume ventilation was significantly associated with lower risk of AF recurrence after 12 months {pooled odds ratio (OR) = 0.62 [95% confidence interval (CI): 0.42-0.92]}, as well as total atrial arrhythmia [OR = 0.59 (95% CI: 0.42-0.81)], with no between-study heterogeneity (<i>I</i> <sup>2</sup> = 0%). Acutely, HFLTV was associated with higher probability of first-pass PVI with borderline statistical significance [OR = 1.24 (95% CI: 0.94-1.63)]. Furthermore, HFLTV was associated with significant reductions in total procedure time [-0.71 (95% CI: -1.00 to -0.42), unit in standard deviation], ablation time [-0.83 (95% CI: -1.07 to -0.59)], and total RF time [-0.72 (95% CI: -0.85 to -0.59)] (heterogeneity <i>I</i> <sup>2</sup> = 76%). Notably, there was no effect modification by paroxysmal or persistent AF (<i>P</i> > 0.05). All studies reported no major complications in either group.</p><p><strong>Conclusion: </strong>High-frequency low-tidal volume ventilation is associated with improved long-term success of arrhythmia control in AF patients who undergo RF catheter ablation, regardless of paroxysmal or persistent status.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf088"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319537/pdf/","citationCount":"0","resultStr":"{\"title\":\"High-frequency low-tidal volume ventilation improves long-term success in radiofrequency catheter ablation of atrial fibrillation: a meta-analysis.\",\"authors\":\"Yap-Hang Will Chan, Hoi-Ying Li, Hung-Fat Tse, Claire A Martin\",\"doi\":\"10.1093/ehjopen/oeaf088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>High-frequency low-tidal volume (HFLTV) ventilation may improve catheter stability and enhance procedural success in radiofrequency (RF) catheter ablation of atrial fibrillation (AF). Long-term findings remained unclear.</p><p><strong>Methods and results: </strong>We conducted a meta-analysis that included all studies that directly compared AF patients who underwent RF ablation under HFLTV compared with standard ventilation. Primary outcomes included acute first-pass pulmonary vein isolation (PVI) and long-term recurrence of AF/atrial arrhythmias after 12 months. Secondary outcomes included total procedure duration, ablation time, and RF time, with pooled standardized mean difference derived using the inverse variance method. Five cohort studies (publication period: 2019-2024) were identified and included in the meta-analysis (final sample: HFLTV <i>n</i> = 460 vs. standard ventilation <i>n</i> = 705). High-frequency low-tidal volume ventilation was significantly associated with lower risk of AF recurrence after 12 months {pooled odds ratio (OR) = 0.62 [95% confidence interval (CI): 0.42-0.92]}, as well as total atrial arrhythmia [OR = 0.59 (95% CI: 0.42-0.81)], with no between-study heterogeneity (<i>I</i> <sup>2</sup> = 0%). Acutely, HFLTV was associated with higher probability of first-pass PVI with borderline statistical significance [OR = 1.24 (95% CI: 0.94-1.63)]. Furthermore, HFLTV was associated with significant reductions in total procedure time [-0.71 (95% CI: -1.00 to -0.42), unit in standard deviation], ablation time [-0.83 (95% CI: -1.07 to -0.59)], and total RF time [-0.72 (95% CI: -0.85 to -0.59)] (heterogeneity <i>I</i> <sup>2</sup> = 76%). Notably, there was no effect modification by paroxysmal or persistent AF (<i>P</i> > 0.05). All studies reported no major complications in either group.</p><p><strong>Conclusion: </strong>High-frequency low-tidal volume ventilation is associated with improved long-term success of arrhythmia control in AF patients who undergo RF catheter ablation, regardless of paroxysmal or persistent status.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 4\",\"pages\":\"oeaf088\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319537/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf088\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
High-frequency low-tidal volume ventilation improves long-term success in radiofrequency catheter ablation of atrial fibrillation: a meta-analysis.
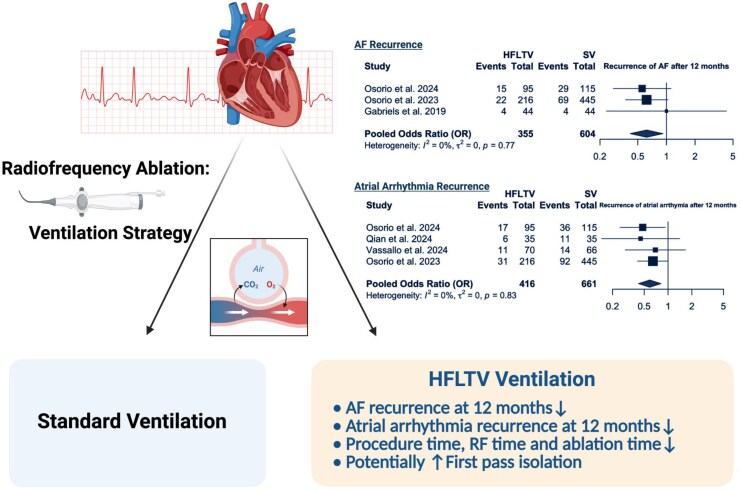
Aims: High-frequency low-tidal volume (HFLTV) ventilation may improve catheter stability and enhance procedural success in radiofrequency (RF) catheter ablation of atrial fibrillation (AF). Long-term findings remained unclear.
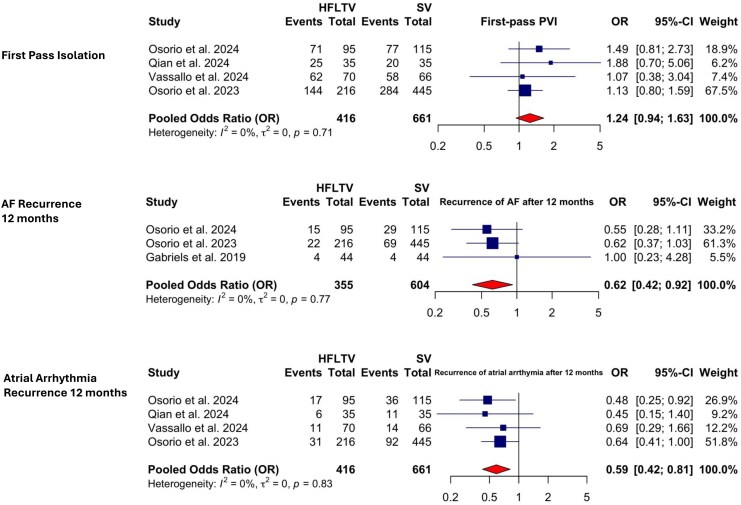
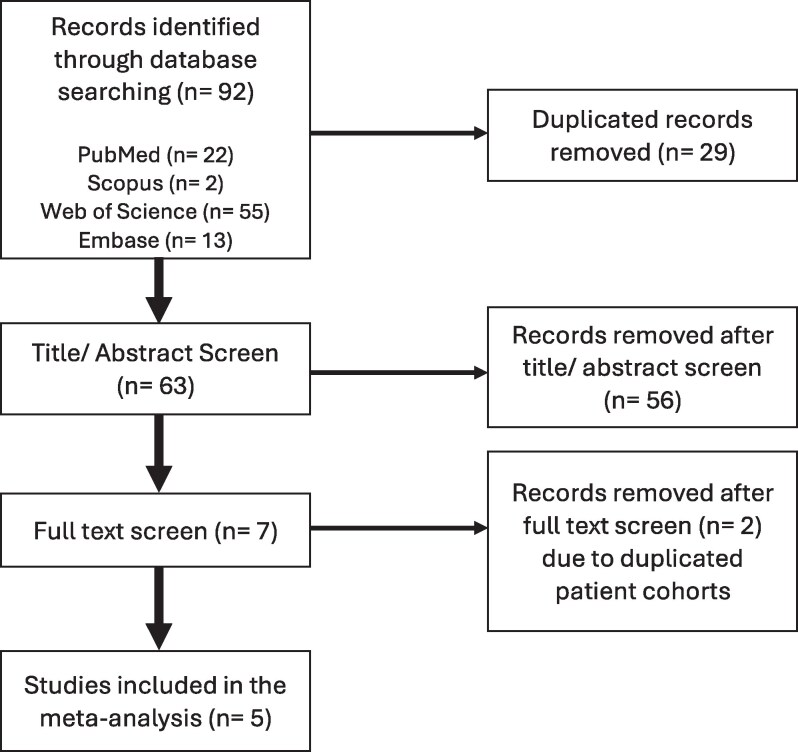
Methods and results: We conducted a meta-analysis that included all studies that directly compared AF patients who underwent RF ablation under HFLTV compared with standard ventilation. Primary outcomes included acute first-pass pulmonary vein isolation (PVI) and long-term recurrence of AF/atrial arrhythmias after 12 months. Secondary outcomes included total procedure duration, ablation time, and RF time, with pooled standardized mean difference derived using the inverse variance method. Five cohort studies (publication period: 2019-2024) were identified and included in the meta-analysis (final sample: HFLTV n = 460 vs. standard ventilation n = 705). High-frequency low-tidal volume ventilation was significantly associated with lower risk of AF recurrence after 12 months {pooled odds ratio (OR) = 0.62 [95% confidence interval (CI): 0.42-0.92]}, as well as total atrial arrhythmia [OR = 0.59 (95% CI: 0.42-0.81)], with no between-study heterogeneity (I2 = 0%). Acutely, HFLTV was associated with higher probability of first-pass PVI with borderline statistical significance [OR = 1.24 (95% CI: 0.94-1.63)]. Furthermore, HFLTV was associated with significant reductions in total procedure time [-0.71 (95% CI: -1.00 to -0.42), unit in standard deviation], ablation time [-0.83 (95% CI: -1.07 to -0.59)], and total RF time [-0.72 (95% CI: -0.85 to -0.59)] (heterogeneity I2 = 76%). Notably, there was no effect modification by paroxysmal or persistent AF (P > 0.05). All studies reported no major complications in either group.
Conclusion: High-frequency low-tidal volume ventilation is associated with improved long-term success of arrhythmia control in AF patients who undergo RF catheter ablation, regardless of paroxysmal or persistent status.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


