Daniel V Araujo, Bruno Lins Souza, Mariana F Seibel, Aline F Fares, Vitor T Liutti
{"title":"达非尼和曲美替尼与抗pd (L)1辅助治疗局部晚期braf突变黑色素瘤:系统回顾和荟萃分析","authors":"Daniel V Araujo, Bruno Lins Souza, Mariana F Seibel, Aline F Fares, Vitor T Liutti","doi":"10.1093/oncolo/oyaf247","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Both dabrafenib and trametinib (D + T) and anti-PD(L)1s have been shown to improve recurrence-free survival (RFS) in patients with stage III or resected stage IV BRAF-mutant melanoma. However, no randomized controlled trials (RCTs) have directly compared them in the adjuvant setting, creating uncertainties about the optimal approach. This systematic review and meta-analysis address this knowledge gap.</p><p><strong>Methods: </strong>A comprehensive search of PubMed, Embase, and Scopus was conducted to identify studies comparing D + T with anti-PD(L)1 therapies. Studies with overlapping populations were excluded. Statistical analyses employed a random-effects model, with heterogeneity assessed via I 2 statistics. This study was registered with PROSPERO (CRD42024553421).</p><p><strong>Results: </strong>Eight observational studies (2394 patients) met the inclusion criteria. No eligible RCTs were identified. Median follow-up ranged from 10 to 53 months. Dabrafenib and trametinib improved RFS compared to anti-PD(L)1 therapies (hazard ratio [HR] 0.53, 95% CI, 0.40-0.70, P < .01; I 2 = 55%). However, no significant difference was observed in overall survival (OS) (HR 0.83, 95% CI, 0.60-1.15, P = .27; I 2 = 0%). Subgroup and sensitivity analyses yielded similar results. Dabrafenib and trametinib was associated with a higher rate of treatment discontinuation due to adverse events (AEs), with a relative risk of 1.57 (95% CI, 1.30-1.91, P < .01; I 2 = 0%), corresponding to a risk difference of 8% (95% CI, 5%-12%, P < .01; I 2 = 0%).</p><p><strong>Conclusions: </strong>Dabrafenib and trametinib demonstrated superiority over anti-PD(L)1 therapies in terms of RFS. However, no OS benefit was observed, and D + T was associated with a higher risk of treatment discontinuation. These findings should be considered when counseling patients, as the choice of adjuvant therapy may need to be tailored to individual preferences and tolerability.</p>","PeriodicalId":54686,"journal":{"name":"Oncologist","volume":" ","pages":""},"PeriodicalIF":4.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449075/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dabrafenib and trametinib vs anti-PD(L)1 for the adjuvant treatment of locally advanced BRAF-mutant melanoma: a systematic review and meta-analysis.\",\"authors\":\"Daniel V Araujo, Bruno Lins Souza, Mariana F Seibel, Aline F Fares, Vitor T Liutti\",\"doi\":\"10.1093/oncolo/oyaf247\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Both dabrafenib and trametinib (D + T) and anti-PD(L)1s have been shown to improve recurrence-free survival (RFS) in patients with stage III or resected stage IV BRAF-mutant melanoma. However, no randomized controlled trials (RCTs) have directly compared them in the adjuvant setting, creating uncertainties about the optimal approach. This systematic review and meta-analysis address this knowledge gap.</p><p><strong>Methods: </strong>A comprehensive search of PubMed, Embase, and Scopus was conducted to identify studies comparing D + T with anti-PD(L)1 therapies. Studies with overlapping populations were excluded. Statistical analyses employed a random-effects model, with heterogeneity assessed via I 2 statistics. This study was registered with PROSPERO (CRD42024553421).</p><p><strong>Results: </strong>Eight observational studies (2394 patients) met the inclusion criteria. No eligible RCTs were identified. Median follow-up ranged from 10 to 53 months. Dabrafenib and trametinib improved RFS compared to anti-PD(L)1 therapies (hazard ratio [HR] 0.53, 95% CI, 0.40-0.70, P < .01; I 2 = 55%). However, no significant difference was observed in overall survival (OS) (HR 0.83, 95% CI, 0.60-1.15, P = .27; I 2 = 0%). Subgroup and sensitivity analyses yielded similar results. Dabrafenib and trametinib was associated with a higher rate of treatment discontinuation due to adverse events (AEs), with a relative risk of 1.57 (95% CI, 1.30-1.91, P < .01; I 2 = 0%), corresponding to a risk difference of 8% (95% CI, 5%-12%, P < .01; I 2 = 0%).</p><p><strong>Conclusions: </strong>Dabrafenib and trametinib demonstrated superiority over anti-PD(L)1 therapies in terms of RFS. However, no OS benefit was observed, and D + T was associated with a higher risk of treatment discontinuation. These findings should be considered when counseling patients, as the choice of adjuvant therapy may need to be tailored to individual preferences and tolerability.</p>\",\"PeriodicalId\":54686,\"journal\":{\"name\":\"Oncologist\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449075/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Oncologist\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/oncolo/oyaf247\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncologist","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/oncolo/oyaf247","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Dabrafenib and trametinib vs anti-PD(L)1 for the adjuvant treatment of locally advanced BRAF-mutant melanoma: a systematic review and meta-analysis.
Background: Both dabrafenib and trametinib (D + T) and anti-PD(L)1s have been shown to improve recurrence-free survival (RFS) in patients with stage III or resected stage IV BRAF-mutant melanoma. However, no randomized controlled trials (RCTs) have directly compared them in the adjuvant setting, creating uncertainties about the optimal approach. This systematic review and meta-analysis address this knowledge gap.
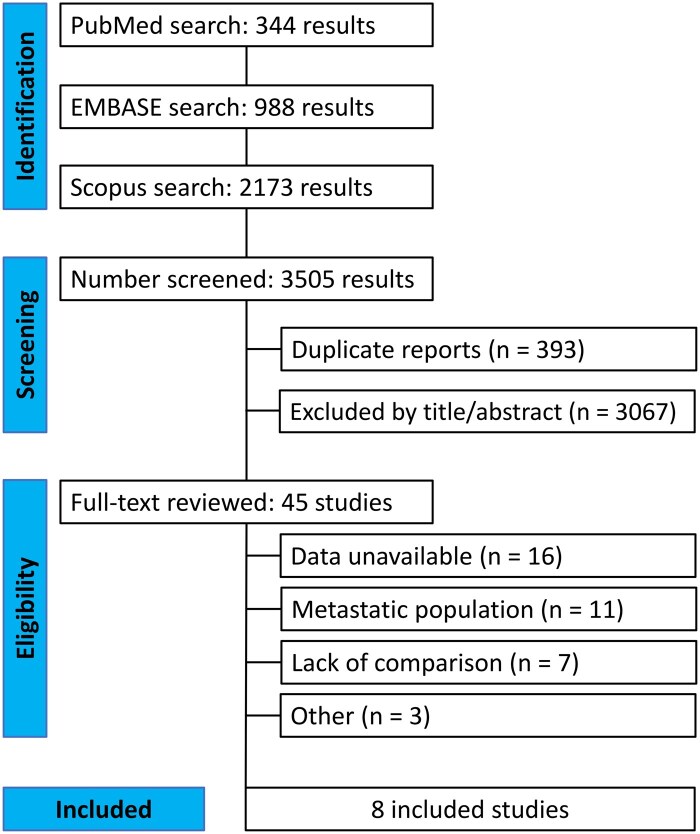
Methods: A comprehensive search of PubMed, Embase, and Scopus was conducted to identify studies comparing D + T with anti-PD(L)1 therapies. Studies with overlapping populations were excluded. Statistical analyses employed a random-effects model, with heterogeneity assessed via I 2 statistics. This study was registered with PROSPERO (CRD42024553421).
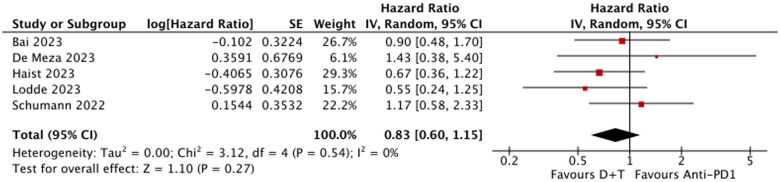
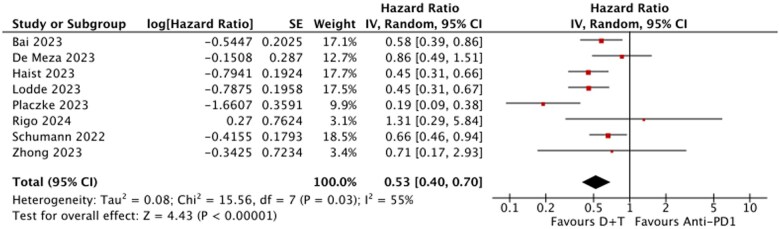
Results: Eight observational studies (2394 patients) met the inclusion criteria. No eligible RCTs were identified. Median follow-up ranged from 10 to 53 months. Dabrafenib and trametinib improved RFS compared to anti-PD(L)1 therapies (hazard ratio [HR] 0.53, 95% CI, 0.40-0.70, P < .01; I 2 = 55%). However, no significant difference was observed in overall survival (OS) (HR 0.83, 95% CI, 0.60-1.15, P = .27; I 2 = 0%). Subgroup and sensitivity analyses yielded similar results. Dabrafenib and trametinib was associated with a higher rate of treatment discontinuation due to adverse events (AEs), with a relative risk of 1.57 (95% CI, 1.30-1.91, P < .01; I 2 = 0%), corresponding to a risk difference of 8% (95% CI, 5%-12%, P < .01; I 2 = 0%).
Conclusions: Dabrafenib and trametinib demonstrated superiority over anti-PD(L)1 therapies in terms of RFS. However, no OS benefit was observed, and D + T was associated with a higher risk of treatment discontinuation. These findings should be considered when counseling patients, as the choice of adjuvant therapy may need to be tailored to individual preferences and tolerability.
期刊介绍:
The Oncologist® is dedicated to translating the latest research developments into the best multidimensional care for cancer patients. Thus, The Oncologist is committed to helping physicians excel in this ever-expanding environment through the publication of timely reviews, original studies, and commentaries on important developments. We believe that the practice of oncology requires both an understanding of a range of disciplines encompassing basic science related to cancer, translational research, and clinical practice, but also the socioeconomic and psychosocial factors that determine access to care and quality of life and function following cancer treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


