Eduardo N Novais, Timothy Borden, Thierry Pauyo, Mariana G Ferrer, Patricia Miller, Maranho Daniel
{"title":"哪一种x线测量能最好地预测单侧股骨干骨骺滑动患者的对侧滑动?","authors":"Eduardo N Novais, Timothy Borden, Thierry Pauyo, Mariana G Ferrer, Patricia Miller, Maranho Daniel","doi":"10.1016/j.jposna.2025.100204","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Managing the contralateral hip in patients with unilateral slipped capital femoral epiphysis (SCFE) involves balancing the risks of prophylactic pinning against the potential for a subsequent slip. This study aimed to evaluate the role of radiographic methods in predicting contralateral slips in patients with unilateral SCFE.</p><p><strong>Methods: </strong>We assessed frog-leg radiographs from 312 patients with unilateral SCFE, measuring the Billings, Southwick, Posterior Sloping Angle (PSA), and tilt angles. Seventy patients (22%) experienced contralateral slips, with a median follow-up of 42 months (range, 18-70 months). Radiographs were evaluated independently by four raters at two separate time points. The radiographic parameters were compared between patients who developed contralateral slips and those who did not, and the diagnostic utility of each radiographic measure was assessed through receiver operating characteristic (ROC) curve analysis, with area under the ROC curve (AUC) values calculated for each method. Sensitivity, specificity, and predictive values were also determined using literature-based cutoffs for the angles (tilt angle >10°, Billings >12°, PSA >14°, Southwick >12°).</p><p><strong>Results: </strong>ROC analysis showed discriminatory ability for all measures, with AUCs ranging from 0.61 to 0.66. The Tilt angle had the highest overall accuracy (77%; 95% CI = 72-82%) and specificity (93%) but the lowest sensitivity (21%). The Billings angle was the most sensitive (83%; 95% CI = 72-92%). All methods displayed good negative predictive values (NPV) between 80 and 90% and excellent interrater (ICC = 0.92-0.99) and intrarater (ICC = 0.84-0.98) reliability.</p><p><strong>Conclusions: </strong>Each radiographic method provides reliable predictive information regarding the risk of contralateral slip in unilateral SCFE. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip. These findings provide valuable guidance for decision-making regarding managing the contralateral hip in patients with unilateral SCFE.</p><p><strong>Key concepts: </strong>1.Radiographic Predictive Measurements for Contralateral SCFE: The study evaluates the diagnostic utility of various radiographic angles (Epiphyseal Tilt, Billing's, Posterior Sloping, and Southwick angle) in predicting contralateral slips in unilateral SCFE cases, highlighting their sensitivity, specificity, and clinical implications.2.Interrater and Intrarater Reliability of radiographic measurements: The study demonstrates excellent interrater and intrarater reliability across all radiographic measurements, emphasizing the consistency and reproducibility of these methods for clinical use.3.Limitations of Current Predictive Radiographic Measurements: The study highlights the limitations of existing radiographic methods in achieving perfect predictive accuracy, advocating for future research to explore advanced imaging techniques like 3D MRI or CT to improve the identification of contralateral slip risk.4.Trade-Off Between Sensitivity and Specificity: The findings emphasize the critical trade-off between minimizing missed contralateral slips versus avoiding unnecessary prophylactic pinning.5.Clinical Decision-Making Guidance: By providing detailed accuracy and predictive values for each measurement, the study offers practical guidance for orthopaedic surgeon. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip.</p><p><strong>Level of evidence: </strong>Level III retrospective cohort study.</p>","PeriodicalId":520850,"journal":{"name":"Journal of the Pediatric Orthopaedic Society of North America","volume":"12 ","pages":"100204"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314171/pdf/","citationCount":"0","resultStr":"{\"title\":\"Which Radiographic Measurements Best Predict Contralateral Slip in Patients Who Undergo Pinning for Unilateral Slipped Capital Femoral Epiphysis?\",\"authors\":\"Eduardo N Novais, Timothy Borden, Thierry Pauyo, Mariana G Ferrer, Patricia Miller, Maranho Daniel\",\"doi\":\"10.1016/j.jposna.2025.100204\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Managing the contralateral hip in patients with unilateral slipped capital femoral epiphysis (SCFE) involves balancing the risks of prophylactic pinning against the potential for a subsequent slip. This study aimed to evaluate the role of radiographic methods in predicting contralateral slips in patients with unilateral SCFE.</p><p><strong>Methods: </strong>We assessed frog-leg radiographs from 312 patients with unilateral SCFE, measuring the Billings, Southwick, Posterior Sloping Angle (PSA), and tilt angles. Seventy patients (22%) experienced contralateral slips, with a median follow-up of 42 months (range, 18-70 months). Radiographs were evaluated independently by four raters at two separate time points. The radiographic parameters were compared between patients who developed contralateral slips and those who did not, and the diagnostic utility of each radiographic measure was assessed through receiver operating characteristic (ROC) curve analysis, with area under the ROC curve (AUC) values calculated for each method. Sensitivity, specificity, and predictive values were also determined using literature-based cutoffs for the angles (tilt angle >10°, Billings >12°, PSA >14°, Southwick >12°).</p><p><strong>Results: </strong>ROC analysis showed discriminatory ability for all measures, with AUCs ranging from 0.61 to 0.66. The Tilt angle had the highest overall accuracy (77%; 95% CI = 72-82%) and specificity (93%) but the lowest sensitivity (21%). The Billings angle was the most sensitive (83%; 95% CI = 72-92%). All methods displayed good negative predictive values (NPV) between 80 and 90% and excellent interrater (ICC = 0.92-0.99) and intrarater (ICC = 0.84-0.98) reliability.</p><p><strong>Conclusions: </strong>Each radiographic method provides reliable predictive information regarding the risk of contralateral slip in unilateral SCFE. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip. These findings provide valuable guidance for decision-making regarding managing the contralateral hip in patients with unilateral SCFE.</p><p><strong>Key concepts: </strong>1.Radiographic Predictive Measurements for Contralateral SCFE: The study evaluates the diagnostic utility of various radiographic angles (Epiphyseal Tilt, Billing's, Posterior Sloping, and Southwick angle) in predicting contralateral slips in unilateral SCFE cases, highlighting their sensitivity, specificity, and clinical implications.2.Interrater and Intrarater Reliability of radiographic measurements: The study demonstrates excellent interrater and intrarater reliability across all radiographic measurements, emphasizing the consistency and reproducibility of these methods for clinical use.3.Limitations of Current Predictive Radiographic Measurements: The study highlights the limitations of existing radiographic methods in achieving perfect predictive accuracy, advocating for future research to explore advanced imaging techniques like 3D MRI or CT to improve the identification of contralateral slip risk.4.Trade-Off Between Sensitivity and Specificity: The findings emphasize the critical trade-off between minimizing missed contralateral slips versus avoiding unnecessary prophylactic pinning.5.Clinical Decision-Making Guidance: By providing detailed accuracy and predictive values for each measurement, the study offers practical guidance for orthopaedic surgeon. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip.</p><p><strong>Level of evidence: </strong>Level III retrospective cohort study.</p>\",\"PeriodicalId\":520850,\"journal\":{\"name\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"volume\":\"12 \",\"pages\":\"100204\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314171/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jposna.2025.100204\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Pediatric Orthopaedic Society of North America","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.jposna.2025.100204","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Which Radiographic Measurements Best Predict Contralateral Slip in Patients Who Undergo Pinning for Unilateral Slipped Capital Femoral Epiphysis?
Background: Managing the contralateral hip in patients with unilateral slipped capital femoral epiphysis (SCFE) involves balancing the risks of prophylactic pinning against the potential for a subsequent slip. This study aimed to evaluate the role of radiographic methods in predicting contralateral slips in patients with unilateral SCFE.
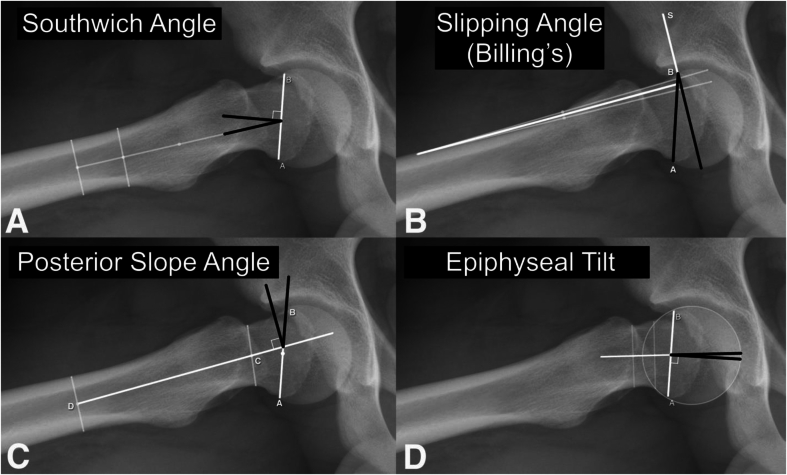
Methods: We assessed frog-leg radiographs from 312 patients with unilateral SCFE, measuring the Billings, Southwick, Posterior Sloping Angle (PSA), and tilt angles. Seventy patients (22%) experienced contralateral slips, with a median follow-up of 42 months (range, 18-70 months). Radiographs were evaluated independently by four raters at two separate time points. The radiographic parameters were compared between patients who developed contralateral slips and those who did not, and the diagnostic utility of each radiographic measure was assessed through receiver operating characteristic (ROC) curve analysis, with area under the ROC curve (AUC) values calculated for each method. Sensitivity, specificity, and predictive values were also determined using literature-based cutoffs for the angles (tilt angle >10°, Billings >12°, PSA >14°, Southwick >12°).
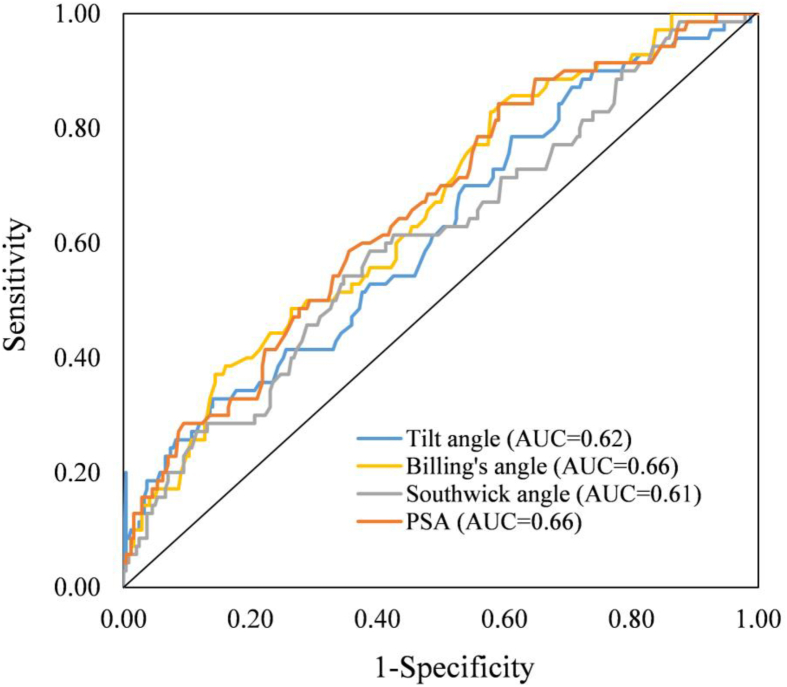
Results: ROC analysis showed discriminatory ability for all measures, with AUCs ranging from 0.61 to 0.66. The Tilt angle had the highest overall accuracy (77%; 95% CI = 72-82%) and specificity (93%) but the lowest sensitivity (21%). The Billings angle was the most sensitive (83%; 95% CI = 72-92%). All methods displayed good negative predictive values (NPV) between 80 and 90% and excellent interrater (ICC = 0.92-0.99) and intrarater (ICC = 0.84-0.98) reliability.
Conclusions: Each radiographic method provides reliable predictive information regarding the risk of contralateral slip in unilateral SCFE. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip. These findings provide valuable guidance for decision-making regarding managing the contralateral hip in patients with unilateral SCFE.
Key concepts: 1.Radiographic Predictive Measurements for Contralateral SCFE: The study evaluates the diagnostic utility of various radiographic angles (Epiphyseal Tilt, Billing's, Posterior Sloping, and Southwick angle) in predicting contralateral slips in unilateral SCFE cases, highlighting their sensitivity, specificity, and clinical implications.2.Interrater and Intrarater Reliability of radiographic measurements: The study demonstrates excellent interrater and intrarater reliability across all radiographic measurements, emphasizing the consistency and reproducibility of these methods for clinical use.3.Limitations of Current Predictive Radiographic Measurements: The study highlights the limitations of existing radiographic methods in achieving perfect predictive accuracy, advocating for future research to explore advanced imaging techniques like 3D MRI or CT to improve the identification of contralateral slip risk.4.Trade-Off Between Sensitivity and Specificity: The findings emphasize the critical trade-off between minimizing missed contralateral slips versus avoiding unnecessary prophylactic pinning.5.Clinical Decision-Making Guidance: By providing detailed accuracy and predictive values for each measurement, the study offers practical guidance for orthopaedic surgeon. Surgeons who aim to minimize the risk of missing a contralateral slip should consider using the Billings angle with a cutoff of 12°, accepting that this may lead to some unnecessary pinning of hips that would not have slipped. Conversely, those who prioritize avoiding unnecessary surgery may prefer the tilt angle with a cutoff of 10°, understanding that this approach could result in missing some hips that will later develop a slip.
Level of evidence: Level III retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


