Gabriella B Smith, Nicole S Pham, Amin Alayleh, Stephanie Smith, Karen Chao, Stuart B Goodman, Kevin G Shea
{"title":"儿童皮质类固醇相关骨坏死的危险因素:一项国家数据库研究。","authors":"Gabriella B Smith, Nicole S Pham, Amin Alayleh, Stephanie Smith, Karen Chao, Stuart B Goodman, Kevin G Shea","doi":"10.1016/j.jposna.2025.100199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse. While the relationship between corticosteroid treatment and osteonecrosis in pediatric patients is well-documented, less is known about which patients are at greatest risk across medical conditions. The purpose of this study was to identify high-risk pediatric populations for developing osteonecrosis following corticosteroid treatment across autoimmune, inflammatory, and oncologic conditions.</p><p><strong>Methods: </strong>The Merative MarketScan Research Databases (2007-2022) were queried to identify pediatric patients with an outpatient oral or intravenous corticosteroid prescription. Demographic, clinical, and prescription differences between osteonecrosis and non-osteonecrosis patients were analyzed using t-tests, Fisher's exact, and chi-square tests. Factors associated with time to osteonecrosis were assessed using a multivariable Cox proportional-hazards regression model.</p><p><strong>Results: </strong>We identified 5,606,781 pediatric patients who received corticosteroids, and 131 developed osteonecrosis. The mean time to osteonecrosis following corticosteroid administration was 7.1 months (SD = 5.2). Osteonecrosis patients were significantly older at the age of corticosteroid administration (12.1 [SD = 4.9] vs. 8.2 [5.6], <i>P</i> < .001) and were prescribed corticosteroids for more total days (136.6 [224.8] vs. 17.1 [89.2], <i>P</i> < .001) compared to patients who did not develop osteonecrosis. Adjusting for all other covariates, risk factors for osteonecrosis include acute lymphoblastic leukemia (HR = 575.82, 95% CI = [346.68, 956.40], <i>P</i> < .001), systemic lupus erythematosus (HR = 106.41, 95% CI = [44.65, 253.63], <i>P</i> < .001), Crohn's disease (HR = 6.67, 95% CI = [1.54, 28.86], <i>P</i> = .011), juvenile idiopathic arthritis (HR = 4.62, 95% CI = [1.06, 20.08], <i>P</i> = .041), solid organ transplant (HR = 4.24, 95% CI = [2.08, 8.65], <i>P</i> < .001), dexamethasone (HR = 2.59, 95% CI = [1.56, 4.28], <i>P</i> < .001), older age (hazard ratio [HR] = 1.11, 95% CI = [1.06, 1.16], <i>P</i> < .001), and greater total days prescribed (HR = 1.01, 95% CI = [1.00, 1.02], <i>P</i> = .041).</p><p><strong>Conclusions: </strong>Our national database study highlights the need for targeted screening of pediatric patients treated with high-dose corticosteroids. This investigation may inform multidisciplinary studies and interventions in children treated with corticosteroids.</p><p><strong>Key concepts: </strong>(1)Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse, yet little is known regarding which pediatric patients are at greatest risk across medical conditions.(2)Adjusting for other covariates, pediatric patients with acute lymphoblastic leukemia, systemic lupus erythematous, Crohn's disease, juvenile idiopathic arthritis, solid organ transplants, patients prescribed dexamethasone, patients prescribed corticosteroids for greater total days, and older patients were at increased risk for osteonecrosis in our national database study.(3)Our findings highlight the need for targeted screening of pediatric patients treated with high-dose corticosteroids.(4)Future prospective multidisciplinary screening and intervention protocols should be studied in children treated with corticosteroids.</p><p><strong>Level of evidence: </strong>Level III: Case-control study or retrospective cohort study.</p>","PeriodicalId":520850,"journal":{"name":"Journal of the Pediatric Orthopaedic Society of North America","volume":"12 ","pages":"100199"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317409/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors for Corticosteroid-associated Osteonecrosis in Children: A National Database Study.\",\"authors\":\"Gabriella B Smith, Nicole S Pham, Amin Alayleh, Stephanie Smith, Karen Chao, Stuart B Goodman, Kevin G Shea\",\"doi\":\"10.1016/j.jposna.2025.100199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse. While the relationship between corticosteroid treatment and osteonecrosis in pediatric patients is well-documented, less is known about which patients are at greatest risk across medical conditions. The purpose of this study was to identify high-risk pediatric populations for developing osteonecrosis following corticosteroid treatment across autoimmune, inflammatory, and oncologic conditions.</p><p><strong>Methods: </strong>The Merative MarketScan Research Databases (2007-2022) were queried to identify pediatric patients with an outpatient oral or intravenous corticosteroid prescription. Demographic, clinical, and prescription differences between osteonecrosis and non-osteonecrosis patients were analyzed using t-tests, Fisher's exact, and chi-square tests. Factors associated with time to osteonecrosis were assessed using a multivariable Cox proportional-hazards regression model.</p><p><strong>Results: </strong>We identified 5,606,781 pediatric patients who received corticosteroids, and 131 developed osteonecrosis. The mean time to osteonecrosis following corticosteroid administration was 7.1 months (SD = 5.2). Osteonecrosis patients were significantly older at the age of corticosteroid administration (12.1 [SD = 4.9] vs. 8.2 [5.6], <i>P</i> < .001) and were prescribed corticosteroids for more total days (136.6 [224.8] vs. 17.1 [89.2], <i>P</i> < .001) compared to patients who did not develop osteonecrosis. Adjusting for all other covariates, risk factors for osteonecrosis include acute lymphoblastic leukemia (HR = 575.82, 95% CI = [346.68, 956.40], <i>P</i> < .001), systemic lupus erythematosus (HR = 106.41, 95% CI = [44.65, 253.63], <i>P</i> < .001), Crohn's disease (HR = 6.67, 95% CI = [1.54, 28.86], <i>P</i> = .011), juvenile idiopathic arthritis (HR = 4.62, 95% CI = [1.06, 20.08], <i>P</i> = .041), solid organ transplant (HR = 4.24, 95% CI = [2.08, 8.65], <i>P</i> < .001), dexamethasone (HR = 2.59, 95% CI = [1.56, 4.28], <i>P</i> < .001), older age (hazard ratio [HR] = 1.11, 95% CI = [1.06, 1.16], <i>P</i> < .001), and greater total days prescribed (HR = 1.01, 95% CI = [1.00, 1.02], <i>P</i> = .041).</p><p><strong>Conclusions: </strong>Our national database study highlights the need for targeted screening of pediatric patients treated with high-dose corticosteroids. This investigation may inform multidisciplinary studies and interventions in children treated with corticosteroids.</p><p><strong>Key concepts: </strong>(1)Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse, yet little is known regarding which pediatric patients are at greatest risk across medical conditions.(2)Adjusting for other covariates, pediatric patients with acute lymphoblastic leukemia, systemic lupus erythematous, Crohn's disease, juvenile idiopathic arthritis, solid organ transplants, patients prescribed dexamethasone, patients prescribed corticosteroids for greater total days, and older patients were at increased risk for osteonecrosis in our national database study.(3)Our findings highlight the need for targeted screening of pediatric patients treated with high-dose corticosteroids.(4)Future prospective multidisciplinary screening and intervention protocols should be studied in children treated with corticosteroids.</p><p><strong>Level of evidence: </strong>Level III: Case-control study or retrospective cohort study.</p>\",\"PeriodicalId\":520850,\"journal\":{\"name\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"volume\":\"12 \",\"pages\":\"100199\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317409/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jposna.2025.100199\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Pediatric Orthopaedic Society of North America","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.jposna.2025.100199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:皮质类固醇相关的骨坏死具有严重疼痛和关节塌陷的风险。虽然皮质类固醇治疗与儿科患者骨坏死之间的关系有充分的文献记载,但在各种医疗条件下,哪些患者的风险最大却鲜为人知。本研究的目的是确定皮质类固醇治疗后发生骨坏死的高危儿童人群,包括自身免疫性、炎症性和肿瘤性疾病。方法:查询Merative MarketScan研究数据库(2007-2022),以确定门诊口服或静脉注射皮质类固醇处方的儿科患者。采用t检验、Fisher精确检验和卡方检验分析骨坏死和非骨坏死患者的人口学、临床和处方差异。使用多变量Cox比例风险回归模型评估与骨坏死时间相关的因素。结果:我们确定了5606781例接受皮质类固醇治疗的儿童患者,其中131例发生了骨坏死。皮质类固醇治疗后发生骨坏死的平均时间为7.1个月(SD = 5.2)。与未发生骨坏死的患者相比,骨坏死患者在使用皮质类固醇的年龄明显更大(12.1 [SD = 4.9]对8.2 [5.6],P < .001),并且使用皮质类固醇的总天数更长(136.6[224.8]对17.1 [89.2],P < .001)。调整了所有其他协变量,骨坏死的风险因素包括急性淋巴细胞白血病(HR = 575.82, 95% CI = [346.68, 956.40], P <措施),系统性红斑狼疮(HR = 106.41, 95% CI = [44.65, 253.63], P <措施),克罗恩病(HR = 6.67, 95% CI = [1.54, 28.86], P = .011),青少年特发性关节炎(HR = 4.62, 95% CI = [1.06, 20.08], P = .041),实体器官移植(HR = 4.24, 95% CI = [2.08, 8.65], P <措施)、地塞米松(HR = 2.59, 95% CI = [1.56, 4.28],P < .001)、年龄越大(风险比[HR] = 1.11, 95% CI = [1.06, 1.16], P < .001)、总处方天数越长(HR = 1.01, 95% CI = [1.00, 1.02], P = .041)。结论:我们的国家数据库研究强调了对接受大剂量皮质类固醇治疗的儿科患者进行针对性筛查的必要性。这项调查可能为使用皮质类固醇治疗儿童的多学科研究和干预提供信息。关键概念:(1)皮质类固醇相关的骨坏死存在严重疼痛和关节塌陷的风险,但在不同的医疗条件下,哪些儿童患者的风险最大尚不清楚。(2)调整其他协变量,急性淋巴细胞白血病、系统性红斑狼疮、克罗恩病、青少年特发性关节炎、实体器官移植的儿童患者,使用地塞米松的患者,使用皮质类固醇总天数较大的患者,(3)我们的研究结果强调了对接受大剂量皮质类固醇治疗的儿童患者进行针对性筛查的必要性。(4)未来的前瞻性多学科筛查和干预方案应在接受皮质类固醇治疗的儿童中进行研究。证据等级:III级:病例对照研究或回顾性队列研究。
Risk Factors for Corticosteroid-associated Osteonecrosis in Children: A National Database Study.
Background: Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse. While the relationship between corticosteroid treatment and osteonecrosis in pediatric patients is well-documented, less is known about which patients are at greatest risk across medical conditions. The purpose of this study was to identify high-risk pediatric populations for developing osteonecrosis following corticosteroid treatment across autoimmune, inflammatory, and oncologic conditions.
Methods: The Merative MarketScan Research Databases (2007-2022) were queried to identify pediatric patients with an outpatient oral or intravenous corticosteroid prescription. Demographic, clinical, and prescription differences between osteonecrosis and non-osteonecrosis patients were analyzed using t-tests, Fisher's exact, and chi-square tests. Factors associated with time to osteonecrosis were assessed using a multivariable Cox proportional-hazards regression model.
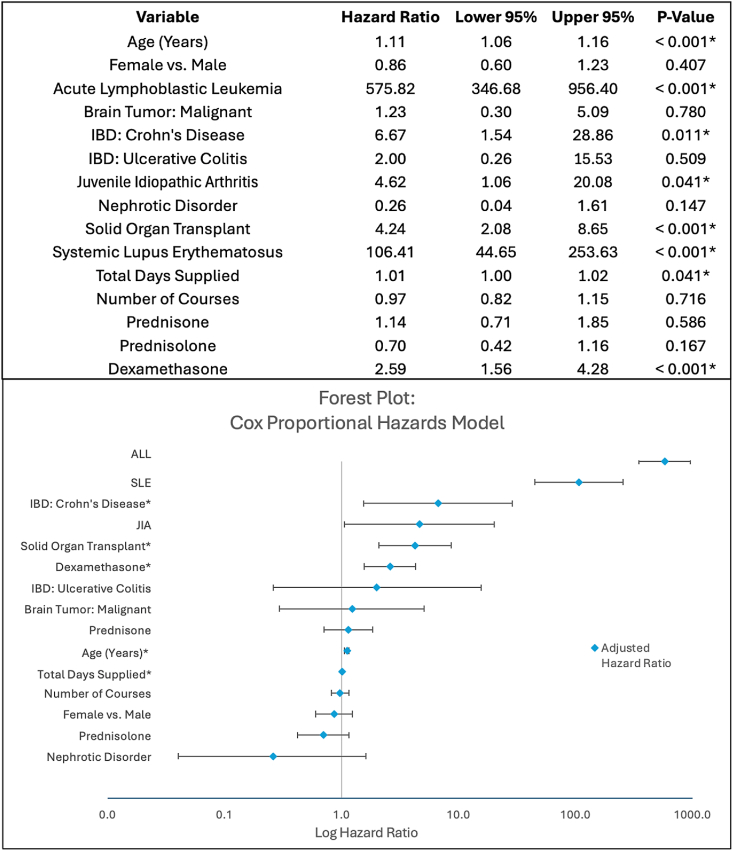
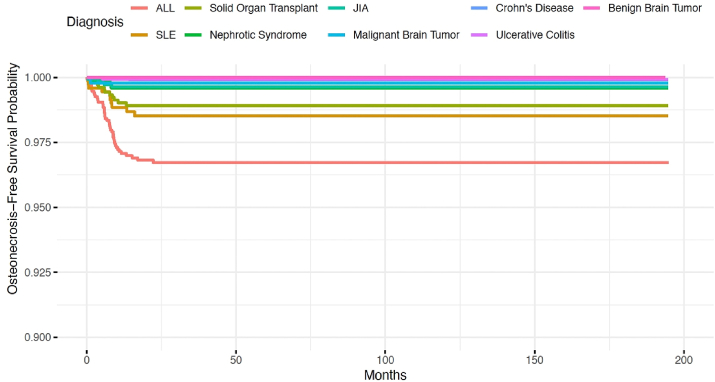
Results: We identified 5,606,781 pediatric patients who received corticosteroids, and 131 developed osteonecrosis. The mean time to osteonecrosis following corticosteroid administration was 7.1 months (SD = 5.2). Osteonecrosis patients were significantly older at the age of corticosteroid administration (12.1 [SD = 4.9] vs. 8.2 [5.6], P < .001) and were prescribed corticosteroids for more total days (136.6 [224.8] vs. 17.1 [89.2], P < .001) compared to patients who did not develop osteonecrosis. Adjusting for all other covariates, risk factors for osteonecrosis include acute lymphoblastic leukemia (HR = 575.82, 95% CI = [346.68, 956.40], P < .001), systemic lupus erythematosus (HR = 106.41, 95% CI = [44.65, 253.63], P < .001), Crohn's disease (HR = 6.67, 95% CI = [1.54, 28.86], P = .011), juvenile idiopathic arthritis (HR = 4.62, 95% CI = [1.06, 20.08], P = .041), solid organ transplant (HR = 4.24, 95% CI = [2.08, 8.65], P < .001), dexamethasone (HR = 2.59, 95% CI = [1.56, 4.28], P < .001), older age (hazard ratio [HR] = 1.11, 95% CI = [1.06, 1.16], P < .001), and greater total days prescribed (HR = 1.01, 95% CI = [1.00, 1.02], P = .041).
Conclusions: Our national database study highlights the need for targeted screening of pediatric patients treated with high-dose corticosteroids. This investigation may inform multidisciplinary studies and interventions in children treated with corticosteroids.
Key concepts: (1)Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse, yet little is known regarding which pediatric patients are at greatest risk across medical conditions.(2)Adjusting for other covariates, pediatric patients with acute lymphoblastic leukemia, systemic lupus erythematous, Crohn's disease, juvenile idiopathic arthritis, solid organ transplants, patients prescribed dexamethasone, patients prescribed corticosteroids for greater total days, and older patients were at increased risk for osteonecrosis in our national database study.(3)Our findings highlight the need for targeted screening of pediatric patients treated with high-dose corticosteroids.(4)Future prospective multidisciplinary screening and intervention protocols should be studied in children treated with corticosteroids.
Level of evidence: Level III: Case-control study or retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


