Apurva S Shah, Zoe E Belardo, Mark L Miller, Michael C Willey, Susan T Mahan, Divya Talwar, Donald S Bae
{"title":"儿童桡骨远端骨折失去复位:来自前瞻性多中心登记的危险因素。","authors":"Apurva S Shah, Zoe E Belardo, Mark L Miller, Michael C Willey, Susan T Mahan, Divya Talwar, Donald S Bae","doi":"10.1016/j.jposna.2025.100206","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Despite numerous single-center studies, uncertainty regarding the management of unstable pediatric distal radius fractures persists. The purpose of this investigation was to report patient factors and fracture characteristics that influence loss of reduction (LOR) or need for secondary procedures following closed reduction of pediatric distal radius fractures in a large, prospective multicenter cohort.</p><p><strong>Methods: </strong>Children aged 4-18 years old undergoing closed reduction for a displaced distal radius fracture were identified from the multicenter Pediatric Distal Radius Fracture (PDRF) Registry. Radiographic LOR was defined as a change in angulation ≥10° or an increase in translation of ≥2 out of 5 categories. Bivariate analysis and multivariate logistic regressions were performed.</p><p><strong>Results: </strong>In total, 616 children (69% male) with a mean age of 10.5 ± 3.4 years were included. The majority of subjects sustained bicortical metaphyseal distal radius fractures (68%), followed by Salter-Harris II physeal fractures (26%). The rate of radiographic LOR was 44% (271/616), and 11% (70/616) of fractures shifted ≥20°. On multivariate analysis, metaphyseal bicortical fracture pattern (OR = 2.3), prereduction translation of ≥51% (OR = 2.3), and nonanatomic closed reductions (OR = 1.9) independently increased the odds of LOR. Patient age, sex, and body mass index (BMI) were not significant predictors for LOR. Ultimately, 8% of children (47/616) underwent secondary procedures, including repeat closed reduction or operative treatment.</p><p><strong>Conclusions: </strong>Redisplacement of pediatric distal radius fractures after closed reduction is common (44%) and is greatly influenced by fracture characteristics. Roughly 11% of fractures will shift ≥20° after closed reduction and 8% undergo secondary procedures. Bicortical fracture pattern, prereduction fracture translation ≥51%, and nonanatomic closed reductions are independent risk factors for redisplacement. Dedicated effort should be made to minimize fracture translation at primary closed reduction, not because of remodeling potential, but to minimize the risk of angulation-driven LOR.</p><p><strong>Key concepts: </strong>(1)Approximately 4 out of 10 pediatric distal radius fractures experience re-displacement after closed reduction and 1 out of 10 will shift ≥20°.(2)Bicortical fracture patterns, prereduction fracture translation ≥51% of the radial shaft width, and nonanatomic closed reductions are independent risk factors for loss of reduction.(3)Any residual fracture translation at the time of closed reduction significantly increases the likelihood of redisplacement.</p><p><strong>Level of evidence: </strong>Level II: Prospective cohort study.</p>","PeriodicalId":520850,"journal":{"name":"Journal of the Pediatric Orthopaedic Society of North America","volume":"12 ","pages":"100206"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317416/pdf/","citationCount":"0","resultStr":"{\"title\":\"Loss of Reduction in Pediatric Distal Radius Fractures: Risk Factors From a Prospective Multicenter Registry.\",\"authors\":\"Apurva S Shah, Zoe E Belardo, Mark L Miller, Michael C Willey, Susan T Mahan, Divya Talwar, Donald S Bae\",\"doi\":\"10.1016/j.jposna.2025.100206\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Despite numerous single-center studies, uncertainty regarding the management of unstable pediatric distal radius fractures persists. The purpose of this investigation was to report patient factors and fracture characteristics that influence loss of reduction (LOR) or need for secondary procedures following closed reduction of pediatric distal radius fractures in a large, prospective multicenter cohort.</p><p><strong>Methods: </strong>Children aged 4-18 years old undergoing closed reduction for a displaced distal radius fracture were identified from the multicenter Pediatric Distal Radius Fracture (PDRF) Registry. Radiographic LOR was defined as a change in angulation ≥10° or an increase in translation of ≥2 out of 5 categories. Bivariate analysis and multivariate logistic regressions were performed.</p><p><strong>Results: </strong>In total, 616 children (69% male) with a mean age of 10.5 ± 3.4 years were included. The majority of subjects sustained bicortical metaphyseal distal radius fractures (68%), followed by Salter-Harris II physeal fractures (26%). The rate of radiographic LOR was 44% (271/616), and 11% (70/616) of fractures shifted ≥20°. On multivariate analysis, metaphyseal bicortical fracture pattern (OR = 2.3), prereduction translation of ≥51% (OR = 2.3), and nonanatomic closed reductions (OR = 1.9) independently increased the odds of LOR. Patient age, sex, and body mass index (BMI) were not significant predictors for LOR. Ultimately, 8% of children (47/616) underwent secondary procedures, including repeat closed reduction or operative treatment.</p><p><strong>Conclusions: </strong>Redisplacement of pediatric distal radius fractures after closed reduction is common (44%) and is greatly influenced by fracture characteristics. Roughly 11% of fractures will shift ≥20° after closed reduction and 8% undergo secondary procedures. Bicortical fracture pattern, prereduction fracture translation ≥51%, and nonanatomic closed reductions are independent risk factors for redisplacement. Dedicated effort should be made to minimize fracture translation at primary closed reduction, not because of remodeling potential, but to minimize the risk of angulation-driven LOR.</p><p><strong>Key concepts: </strong>(1)Approximately 4 out of 10 pediatric distal radius fractures experience re-displacement after closed reduction and 1 out of 10 will shift ≥20°.(2)Bicortical fracture patterns, prereduction fracture translation ≥51% of the radial shaft width, and nonanatomic closed reductions are independent risk factors for loss of reduction.(3)Any residual fracture translation at the time of closed reduction significantly increases the likelihood of redisplacement.</p><p><strong>Level of evidence: </strong>Level II: Prospective cohort study.</p>\",\"PeriodicalId\":520850,\"journal\":{\"name\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"volume\":\"12 \",\"pages\":\"100206\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317416/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Pediatric Orthopaedic Society of North America\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jposna.2025.100206\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Pediatric Orthopaedic Society of North America","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.jposna.2025.100206","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Loss of Reduction in Pediatric Distal Radius Fractures: Risk Factors From a Prospective Multicenter Registry.
Objectives: Despite numerous single-center studies, uncertainty regarding the management of unstable pediatric distal radius fractures persists. The purpose of this investigation was to report patient factors and fracture characteristics that influence loss of reduction (LOR) or need for secondary procedures following closed reduction of pediatric distal radius fractures in a large, prospective multicenter cohort.
Methods: Children aged 4-18 years old undergoing closed reduction for a displaced distal radius fracture were identified from the multicenter Pediatric Distal Radius Fracture (PDRF) Registry. Radiographic LOR was defined as a change in angulation ≥10° or an increase in translation of ≥2 out of 5 categories. Bivariate analysis and multivariate logistic regressions were performed.
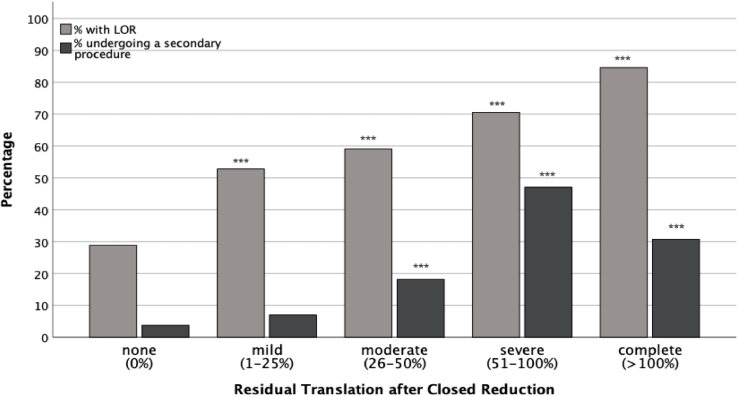
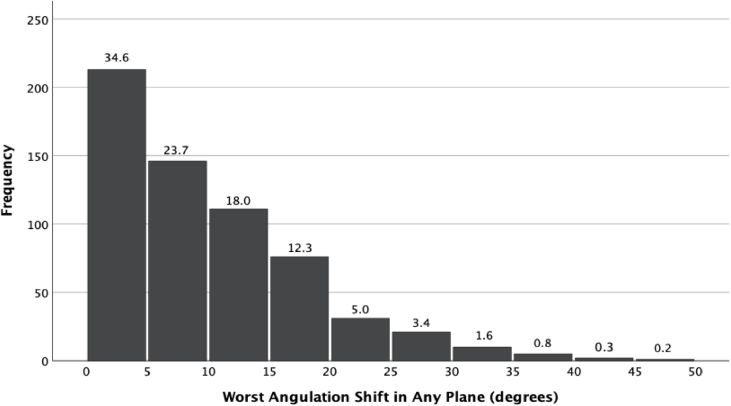
Results: In total, 616 children (69% male) with a mean age of 10.5 ± 3.4 years were included. The majority of subjects sustained bicortical metaphyseal distal radius fractures (68%), followed by Salter-Harris II physeal fractures (26%). The rate of radiographic LOR was 44% (271/616), and 11% (70/616) of fractures shifted ≥20°. On multivariate analysis, metaphyseal bicortical fracture pattern (OR = 2.3), prereduction translation of ≥51% (OR = 2.3), and nonanatomic closed reductions (OR = 1.9) independently increased the odds of LOR. Patient age, sex, and body mass index (BMI) were not significant predictors for LOR. Ultimately, 8% of children (47/616) underwent secondary procedures, including repeat closed reduction or operative treatment.
Conclusions: Redisplacement of pediatric distal radius fractures after closed reduction is common (44%) and is greatly influenced by fracture characteristics. Roughly 11% of fractures will shift ≥20° after closed reduction and 8% undergo secondary procedures. Bicortical fracture pattern, prereduction fracture translation ≥51%, and nonanatomic closed reductions are independent risk factors for redisplacement. Dedicated effort should be made to minimize fracture translation at primary closed reduction, not because of remodeling potential, but to minimize the risk of angulation-driven LOR.
Key concepts: (1)Approximately 4 out of 10 pediatric distal radius fractures experience re-displacement after closed reduction and 1 out of 10 will shift ≥20°.(2)Bicortical fracture patterns, prereduction fracture translation ≥51% of the radial shaft width, and nonanatomic closed reductions are independent risk factors for loss of reduction.(3)Any residual fracture translation at the time of closed reduction significantly increases the likelihood of redisplacement.
Level of evidence: Level II: Prospective cohort study.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


